
CASE HISTORY
A 5-year-old male child presented with complaints of recurrent generalized tonic–clonic seizures and right-sided weakness ,predominantly involving the lower limb along with anger outbursts and abnormal behaviour.
No history of fever, head trauma, vision loss, sensory loss, or headache.
No family history of seizure disorder or chronic neurological illness.
Birth history: Full-term normal vaginal delivery, birth weight 2.8 kg, no NICU stay
CASE CONTRIBUTED BY-
Dr Somya Gupta – 3rd year Resident , Department of Radiodiagnosis, Kalinga Institute of Medical Sciences , Bhubaneswar , Odisa
Dr. Tapas kumar sahu , Assistant Professor ,Department of Radiodiagnosis, Kalinga Institute of Medical Sciences , Bhubaneswar , Odisa
Dr. Basanta Manjari Swain (HOD and Professor),Department of Radiodiagnosis, Kalinga Institute of Medical Sciences , Bhubaneswar , Odisa
DESCRIPTION
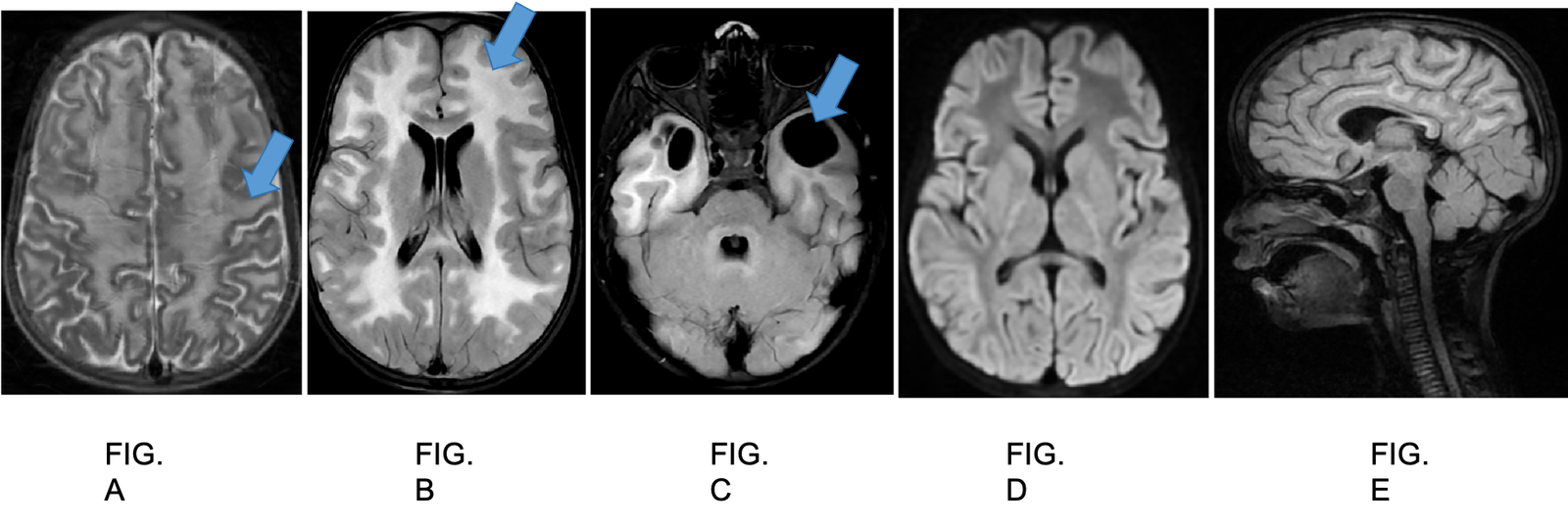
A and B :Axial section of T2 sequence and axial section of FLAIR sequence shows a diffuse, symmetrical hyperintensity in bilateral cerebral white matter including subcortical U-fiberss. The white matter appears swollen, without significant volume loss. Relative sparing of deep white matter
C: Axial FLAIR sequence shows few well-defined subcortical cysts in the anterior temporal lobes bilaterally
D: Axial section of Diffusion weighted sequence shows no abnormality
E: 3D Sagittal cube FLAIR FS sequence shows relatively increased fronto-occipital dimension, consistent with macrocephaly .
Diagnosis:Megalencephalic Leukoencephalopathy with Subcortical Cysts (MLC), also known as Van der Knaap disease
Background
Megalencephalic Leukoencephalopathy with Subcortical Cysts (MLC), also known as Van der Knaap disease, is a rare inherited leukodystrophy .
It follows predominantly an autosomal recessive inheritance pattern
Pathophysiology
MLC is caused by mutations in:
MLC1 (≈75% cases)
HEPACAM (≈20% cases)
These genes encode proteins involved in astrocytic membrane function and regulation of brain water and ion homeostasis.
Defective astrocyte function leads to: Impaired ion and water regulation leading to white matter swelling
,vacuolation of myelin and Formation of subcortical cysts
The disease produces intramyelinic vacuolation rather than primary demyelination.
Classical Features
Macrocephaly (at birth or infancy; earliest and most consistent sign)
Delayed motor milestones
Early-onset seizures Mild early cognitive impairment with progressive Ataxia ,Spasticity ,Dysarthria
Key MRI Findings
Diffuse bilateral symmetric T2/FLAIR hyperintensity of subcortical and deep white matter with corresponding T1 hypointensity
“Swollen white matter” appearance in early stage
Relative sparing of deep grey nuclei and brainstem
Subcortical cysts, predominantly in: Anterior temporal lobes (classical) and Frontoparietal regions
Structures Typically Spared:
Basal ganglia
Thalami
Brainstem
Cerebellar white matter (early stage)
Diffusion Imaging: Usually no true diffusion restriction
Differential Diagnosis-
Canavan disease
Alexander disease
metachromatic leukodystrophy
others causes of megalencephaly
other leukoencephalopathies
References
1) Roy U, Joshi B, Ganguly G. Van der Knaap disease: a rare disease with atypical features. BMJ Case Rep. 2015 Jul 22;2015:bcr2015209831. doi:10.1136/bcr-2015-209831.
2) Jhancy M, Al Homsi A, Chowdhury F, Hossain S, Ahamed R. Van der Knaap Disease (Vanishing White Matter) – Unusual Presentation in a Neonate: A Case Report. Neurol India. 2020 May-Jun;68(3):669-672. doi:10.4103/0028-3886.289018.
3) Das S, Dhibar T. Van der Knaap Disease: A Case Series Highlighting Clinical and Radiological Features. Int J Anat Radiol Surg. 2025 Sep;14(5):RS01-RS03. doi:10.7860/IJARS/2025/81128.3062
Add a Comment
You must be logged in to post a comment