
CASE HISTORY
45 YEAR OLD MALE
Presenting compaints: Patient presented with lower back pain since 5 years; right leg numbness and tingling since 6 months and acute onset urinary incontinence
Past history and comorbidities : H/o pulmonary TB and TB meningitis 15 years ago, completed ATT; Hypertensive since 1 year , on medication.
Physical examination: Unremarkable, with a full range of motion of the cervical and lumbar spine with no pain elicited on movement.
Full strength in both legs with diminished sensation to touch in the right leg and foot in a non-dermatomal distribution.
Reflexes were elevated at the lower extremities bilaterally, but no clonus or Babinski sign was detected.
Workup: Patient was referred for a lumbar spine MR
CASE CONTRIBUTED BY
Dr. MEGHANA KANCHARLA, SENIOR RESIDENT, ST JOHNS MEDICAL COLLEGE AND HOSPITAL
Dr. STALLON SEBASTIAN, ASSISTANT PROFESSOR, ST JOHNS MEDICAL COLLEGE AND HOSPITAL
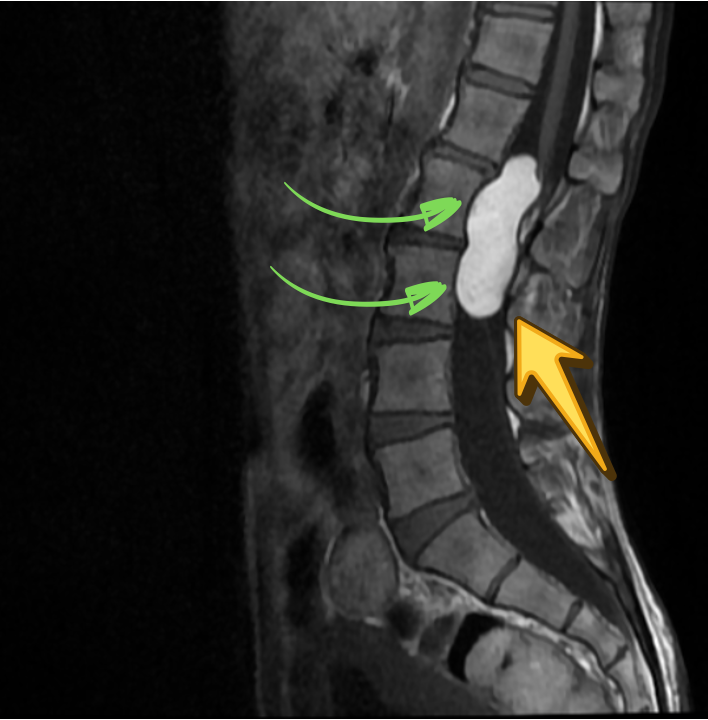
SAGITTAL T2

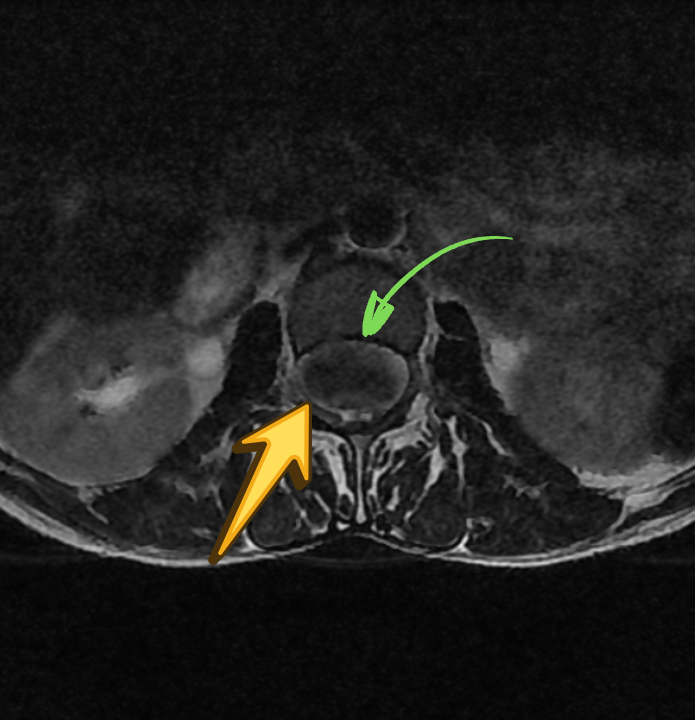
AXIAL T2
SAGITTAL T1
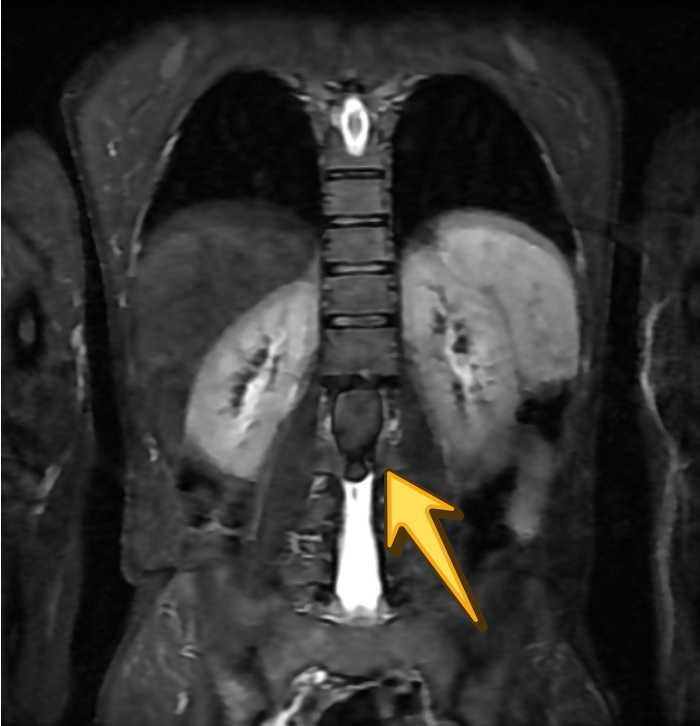
CORONAL T2 STIR
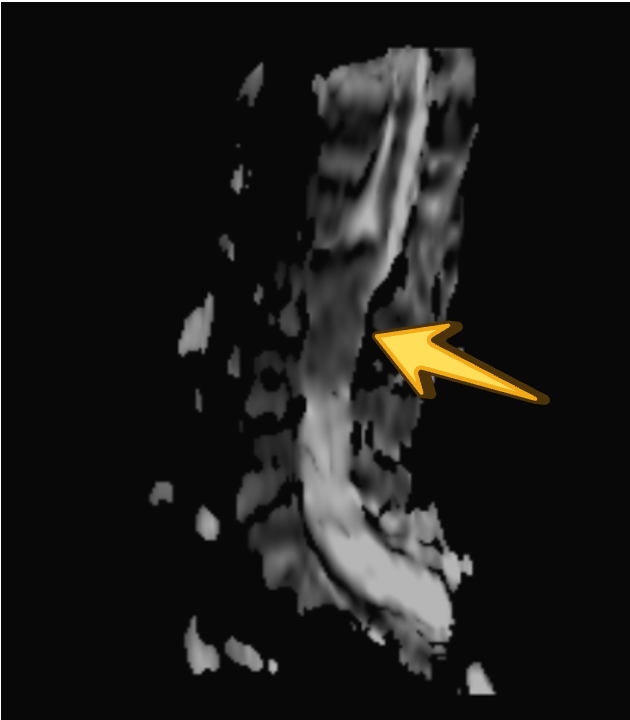
DWI
ADC
T1 PRE CON

T1 POST CON
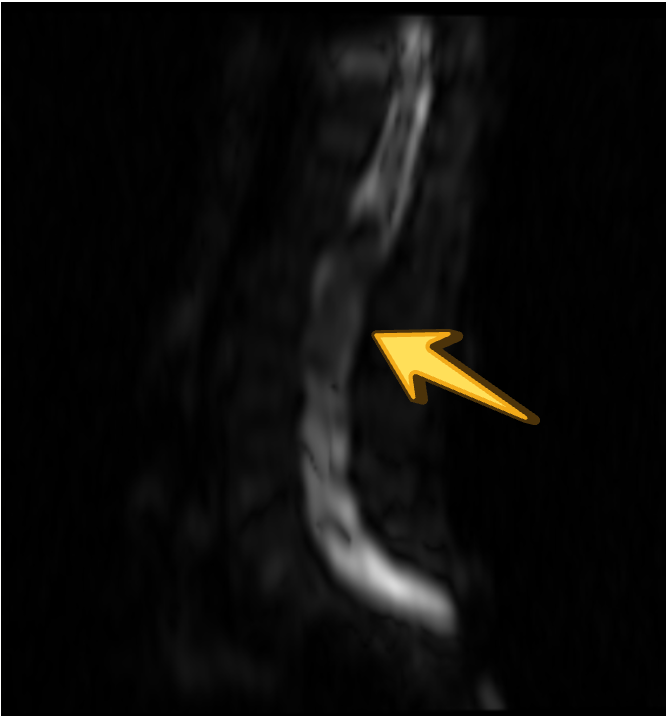
FAT PHASE

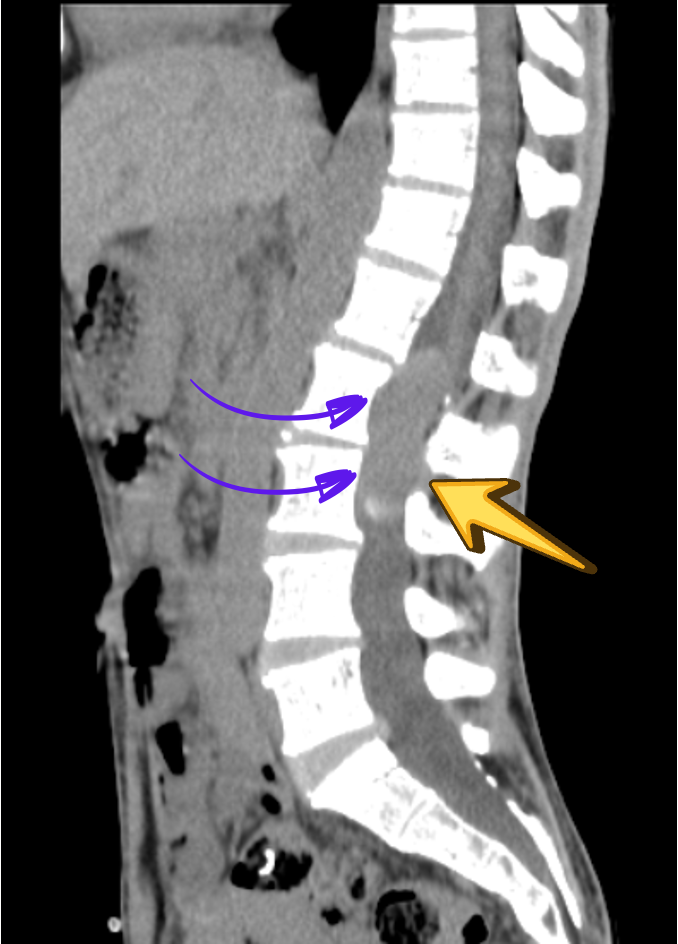
CT
INPHASE

Diagnosis: Atypical Spinal Epidermoid Cyst
Clinical diagnosis:
L2 L3 IDEM
? Lipoma
Gross Description:
Bottle contains 1 irregular piece of grey white soft tissue measures 4×1.8×0.5cm
2 bits embed all – A
Bottle contains <0.25gms of grey white soft tissue
<0.25gms embed all – B
Grossed By – Dr. Deepthi Benny
Microscopy:
- Section shows portions of cyst lined by stratified squamous epithelium. Cyst wall is composed of fibrocollagenous tissue and lymphoplasmacytic infiltrate, admixed with pigment-laden macrophages. Also noted are areas of calcification and congested blood vessels.
- Section shows lamilated keratin flakes
Impression:
Consistent with epidermoid cyst, L2L3 IDEM
DISCUSSION:
Background
Spinal epidermoid cysts are rare, benign, slow-growing intradural lesions arising from ectodermal inclusions, either congenital or acquired following lumbar puncture, spinal surgery, or trauma. They account for <1% of spinal tumors and most commonly involve the lumbar and lumbosacral regions. Due to their indolent growth, patients typically present with long-standing symptoms, which may progress to radiculopathy and sphincter dysfunction.
Imaging
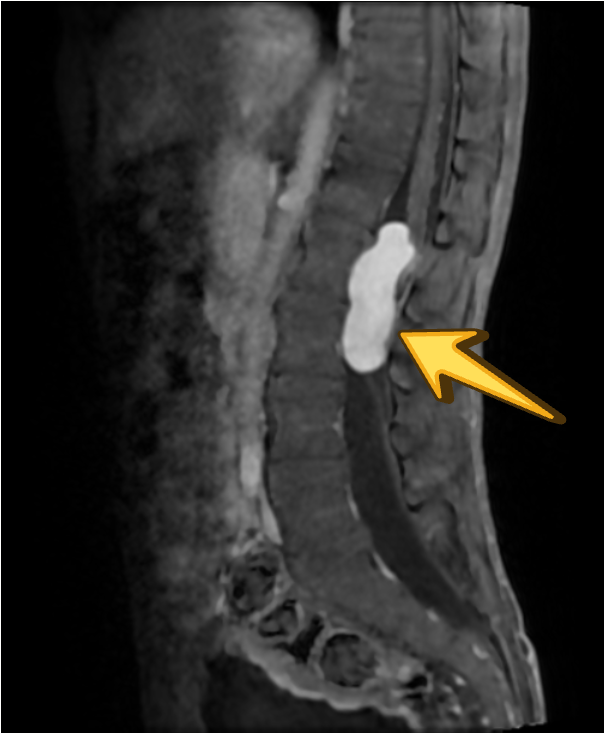
MRI is the modality of choice for evaluation of spinal epidermoid cysts. Although classically described as T1 hypointense, T2 hyperintense lesions with diffusion restriction, imaging appearances may be variable, particularly in chronic or protein-rich lesions.
In the present case, the lesion demonstrates T1 hyperintensity and T2 hypointensity, an atypical appearance attributed to dense keratinaceous debris, cholesterol crystals, high protein concentration, and chronic desiccation, resulting in shortening of T1 and T2 relaxation times. Such lesions are described as atypical or “white” epidermoid cysts.
While diffusion restriction is a characteristic feature, its absence does not exclude the diagnosis, especially in long-standing lesions with compact internal contents and in the setting of technical limitations of spinal diffusion imaging.
Dixon fat-phase imaging demonstrates absence of fat signal, effectively excluding a dermoid cyst and supporting the diagnosis of an epidermoid cyst.
Post-contrast imaging shows no significant internal enhancement, supporting a non-neoplastic cystic etiology.
Associated scalloping of the lumbar vertebral bodies reflects chronic, slow-growing mass effect, further supporting the benign and indolent nature of the lesion.
The imaging differential diagnosis includes dermoid cyst, arachnoid cyst, subacute hemorrhage, melanin-containing lesions, and cystic neoplasms, which were considered less likely based on signal characteristics, lack of fat suppression signal drop, minimal enhancement, chronicity, and histopathological confirmation.
Management
Surgical excision is the treatment of choice. Complete resection may be limited by capsular adherence to neural structures, particularly in chronic lesions, and subtotal excision may predispose to recurrence. Overall, clinical outcomes are favorable following adequate surgical decompression.
Conclusion
•In a patient with long-standing, slowly progressive neurological symptoms, including radiculopathy and sphincter involvement, a benign, indolent intradural pathology should be strongly considered.
•Atypical MRI signal characteristics (T1 hyperintensity, T2 hypointensity) do not exclude spinal epidermoid cyst, particularly in chronic, protein-rich lesions.
•Absence of diffusion restriction, lack of significant enhancement, and associated vertebral scalloping favor a long-standing benign cystic lesion over aggressive or neoplastic etiologies.
•Awareness of imaging variability in chronic epidermoid cysts and correlation with clinical course and histopathology are essential to avoid misdiagnosis.
Add a Comment
You must be logged in to post a comment