
CASE HISTORY
A 41-year-old male came with complaints of back pain radiating to both lower limbs which was gradually progressive, worsened on walking. Paresthesia in both lower limbs for 3 months. He developed urinary incontinence and constipation for 2 months.
There was no history of fever, cough, weight loss or loss of appetite. There was no history of trauma. On examination there was absent ankle jerk bilaterally and S1-S5 hypoaesthesia with perianal sensory loss.
Chest radiograph and abdominal screening showed no abnormality.
A plain CT and CE-MRI of the sacral spine were performed.
INVESTIGATIONS
Hb- 13.0 g/dl (normal). TLC: 10.2 x 109/L (elevated). ESR: 73mm/ 1st hour (elevated). CRP: 9.2 mg/ L (elevated). LDH : 156 U/L (normal).
AUTHORS
Dr. Anusha Shree Thaneeru, Department of Radiology, Manipal Hospitals, Kanakapura Road, Bangalore.
Dr. Sharath Kumar G G, Lead Consultant, Interventional Neuroradiology, Manipal Hospitals, Kanakapura Road, Bangalore.
Dr. Veekshit Shetty, Consultant Neurosurgery, Manipal Hospitals, Kanakapura Road, Bangalore.
Dr. Vidya. M. N., Lead Consultant Pathologist, Manipal hospitals, Old airport Road, Bangalore.
DESCRIPTION
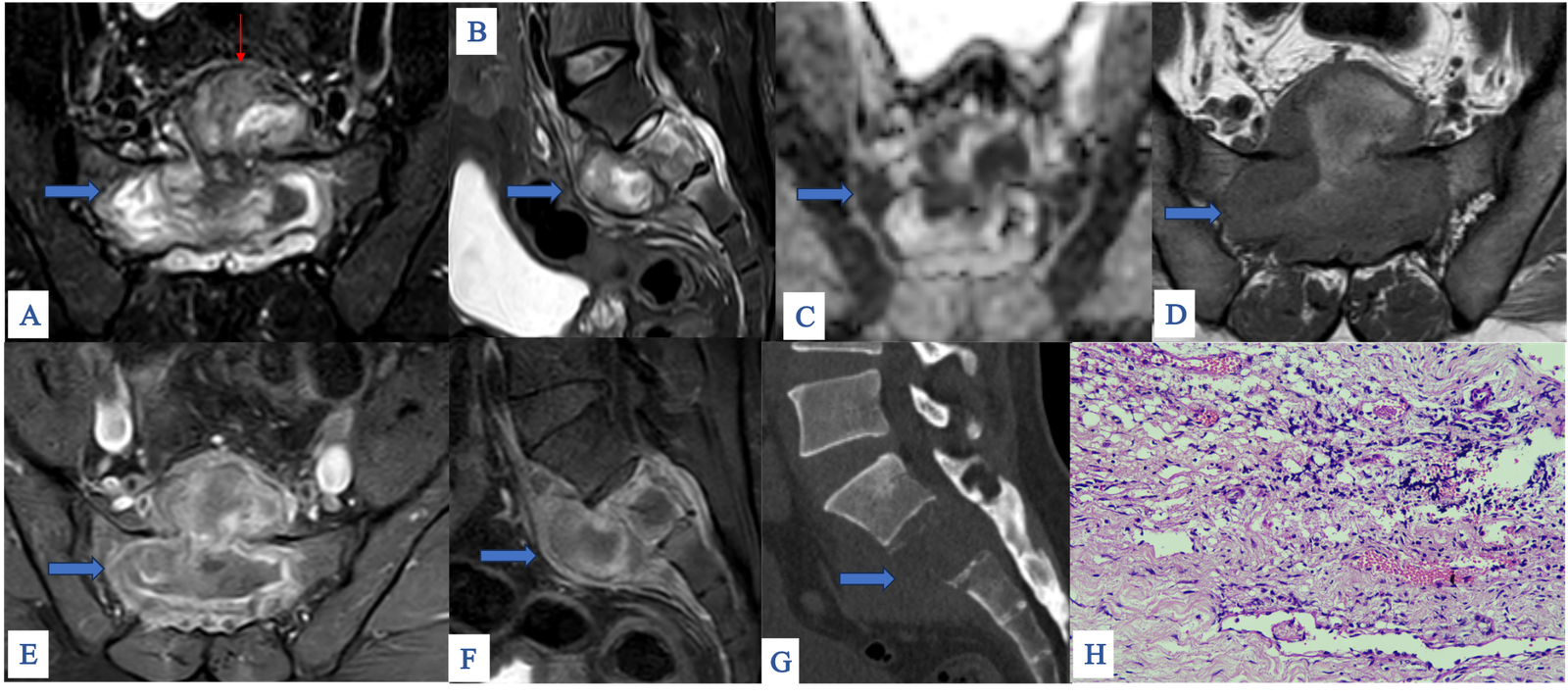
• A & B : Axial and sagittal STIR images showing hyperintense lesion involving the S2 vertebral body (blue arrow) with heterogenous soft tissue component (red arrow). Adjacent bone marrow edema seen.
• C : Areas of diffusion restriction seen within the S2 vertebral body lesion and the presacral soft tissue component.
• D : Axial T1 pre contrast image shows T1 hypointensity.
• E & F : Axial and sagittal T1 post contrast images showing heterogenous enhancement of the lesion.
• G : Sagittal CT images in bone window showing osteolysis involving the S2 vertebral body. No foci of calcification seen within the lesion.
• H : Histopathology slide -shows chronic granulation tissue. Proliferating capillaries are seen with extravasated RBC’s and chronic inflammation.
FINAL DIAGNOSIS
A Granulomatous masquerade – Central body type sacral tuberculosis mimicking neoplasm.
FURTHER MANAGEMENT:
• The patient underwent S1-S2 decompression laminectomy, lumbosacral- iliac fixation using L5. Biopsy of S2 vertebral body lesion was obtained for histopathological evaluation.
• Intraoperatively, there was destruction of S2 vertebral body, replaced by granulation tissue.
• Mycobacteria were detected on Gene Xpert and acid-fast bacilli stain showed scanty bacilli.
• Post surgery patient was started on antitubercular therapy.
DISCUSSION:
• Osteoarticular tuberculosis accounts of 2 to 5% of all tuberculosis cases. The lower thoracic and lumbar spine are the most involved sites. The sacrum and cervical spine are rarely involved1.
• Spinal tuberculosis is almost always due to hematogenous spread of mycobacteria from primary foci in the lungs and/or urogenital tract2.
• The paravertebral venous plexus of Batson is generally thought to be the primary route of spread into the spine. The most common presenting symptoms include discharging sinuses and abscesses in young, sciatic pain and low back pain in adults.
IMAGING CHARACTERISTICS :
Four common imaging patterns of spinal tuberculosis are – paradiscal, central, anterior subligamentous and posterior types 4.
• Paradiscal type is the most common pattern and involved the vertebral bodies adjacent to the intervertebral disc with early involvement of the disc.
• Central type is characterized by involvement of the central vertebral body. It is considered atypical form as the disc is spared breaking the paradigm of paradiscal type where there is early involvement of the intervertebral disc.
• Subligamentous type is spread of infection beneath the anterior longitudinal ligament.
• Posterior element involvement is rare.
Plain radiograph: Very insensitive. May show nonspecific features like osteopenia, loss of definition of vertebral end plate. Cold abscesses may be visible as peri-vertebral soft tissue densities .
CT: Computed tomography is better at delineating bone destruction. It can demonstrate paravertebral abscess and enhancing granulation tissue.
MRI: It is the imaging modality of choice. It allows for early detection of disease before bony deformity occurs. Inflammatory marrow edema appears hypointense on T1-weighted imaging and hyperintense on STIR and T2-weighted imaging showing heterogenous enhancement. Disc involvement is seen as reduced disc space, high T2 signal and contrast enhancement. Phlegmon and cold abscess appear hyperintense on T2 weighted images and hypo-intensity on T1 weighted images. On post contrast T1 weighted images, phlegmon shows uniform enhancement and cold abscess show peripheral enhancement.
MANAGEMENT: Includes primary therapy ATT. Surgical decompression.
DIFFERENTIAL DIAGNOSIS: Primary sacral tumors like chordoma and giant cell tumor.
CONCLUSION:
• Considering the significant overlap in imaging features between atypical central type of tuberculosis involving the sacrum and primary tumors, a high clinical suspicion for tuberculosis is important especially in endemic regions.
• A definitive diagnosis requires histopathological confirmation through biopsy or fine needle aspiration cytology to identify Mycobacterium tuberculosis.
• Initiating antitubercular chemotherapy on time is often effective in treatment and prevention of permanent neurological damage and hence extensive surgeries can be avoided.
| TUBERCULOSIS | CHORDOMA | GIANT CELL TUMOR | |
| Etiology and epidemiology | Infective etiology, common in young adults. | Most common primary malignant tumor of sacrum. Peak incidence in the 5th decade with male preponderance. (5) | Bening but locally aggressive tumor. Incidence between 20-40 years. |
| Characteristics | Often paracentral with adjacent disc involvement. | Midline slow growing sacral mass. Lower sacral vertebrae are commonly involved. | Typically, eccentric lesion involving the upper sacral vertebrae. Fast local expansion to involve the sacroiliac joint. |
| Imaging findings: | Mainly lytic lesion with marginal sclerosis. Calcification and hemorrhagic component – rare. | Purely lytic destructive lesion. Calcifications are common “rings and arcs”. | Expansile lytic lesion. No mineralized matrix. May show cystic changes, fluid-fluid level (ABC like changes). |
| MRI findings: | Heterogenous lesion with cold abscess showing rim enhancement. Disc involvement common. | T2 hyperintense midline lobulated mass with soft tissue extension. | A solid heterogenous mass with extension into adjacent bones. Less T2 hyperintense than chordoma. |
| Soft tissue component | Cold abscess – common. | Large soft tissue component. | Significant soft tissue extension with cortical breakthrough. |
| Investigations | Elevated ESR, CRP. | Usually normal. | Usually normal. |
REFERENCES
1. Shantanu K, Sharma V, Kumar S, Jain S. Tuberculosis of sacrum mimicking as malignancy.
2. Patankar T, Krishnan A, Patkar D, Kale H, Prasad S, Shah J, et al. Imaging in isolated sacral tuberculosis: a review of 15 cases. Skeletal Radiol. 2000;29:392–6. doi:10.1007/s002560000229.
3. Pun WK, Chow SP, Luk KDK, Cheng CL, Hsu LCS, Leong JCY. Tuberculosis of the lumbosacral junction: long term follow-up of 26 cases. J Bone Joint Surg Br 1990; 72:675–678.
4. Vijay Kubihal, Raju Sharma, RG Krishna Kumar, SH Chandrashekara, Rakesh Garg. Imaging update in spinal tuberculosis. DOI: 10.1016/j.jcot.2021.101742
5. Gerber S, Ollivier L, Leclère J, et al. Imaging of sacral tumours. Skeletal Radiol 2008;37:277–89
Add a Comment
You must be logged in to post a comment