
CASE HISTORY
60-year-old adult, chronic smoker with history of angioplasty, presented with recent onset hemoptysis, weight loss and generalized fatigue with mild fever.
CECT Thorax revealed an irregular spiculated mass in the right lung upper lobe.
Underwent CT guided lung biopsy for the same.
Patient developed left sided hemiparesis immediately post procedure with a power of 4/5 in both left upper and lower limb.
Patient was started on 100% O2, he regained full power in both upper and lower limb within 24hrs.
CASE CONTRIBUTED BY
Dr. Jose Siju, MD, Senior Resident, Department of Radiodiagnosis, Tata Memorial Hospital, Mumbai
Dr. Rajas Thaker, MD DNB DM, Senior Resident, Department of Radiodiagnosis, Tata Memorial Hospital, Mumbai
Dr. Varun Yadav, MD FIVR PDCC, Consultant, Department of Radiodiagnosis, Homi Bhabha Cancer Hospital & Research Center, Mullanpur
Day 1
T2 FLAIR

POST CONTRAST T1 FLAIR
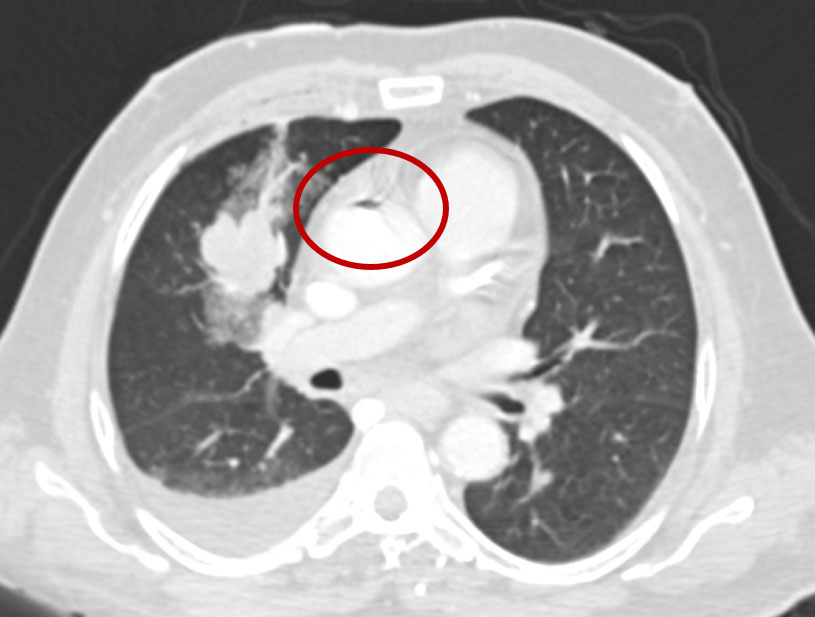
Non-contrast Thorax:
Focus of air in the ascending aorta
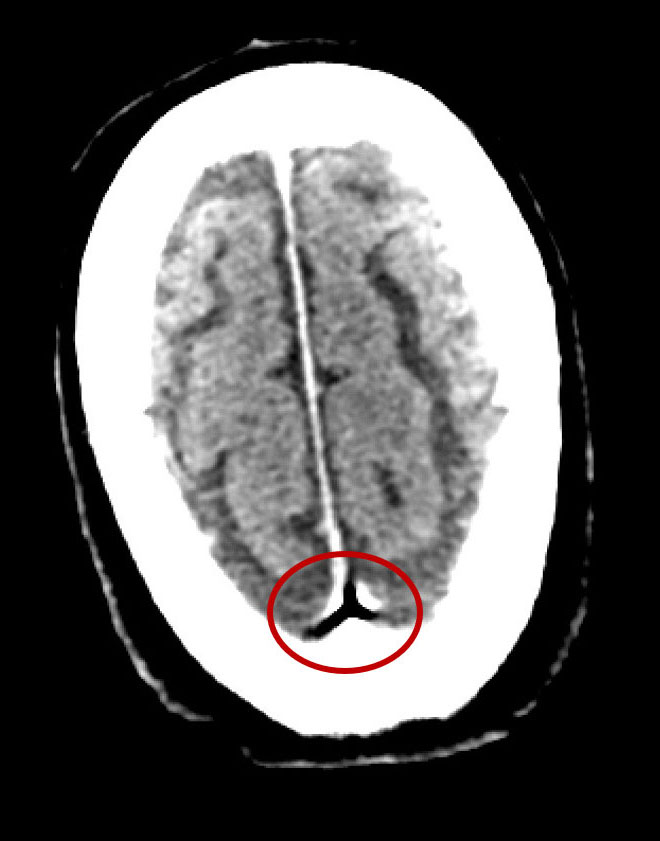
Non-contrast CT Brain:
Focus of air in the superior sagittal sinus
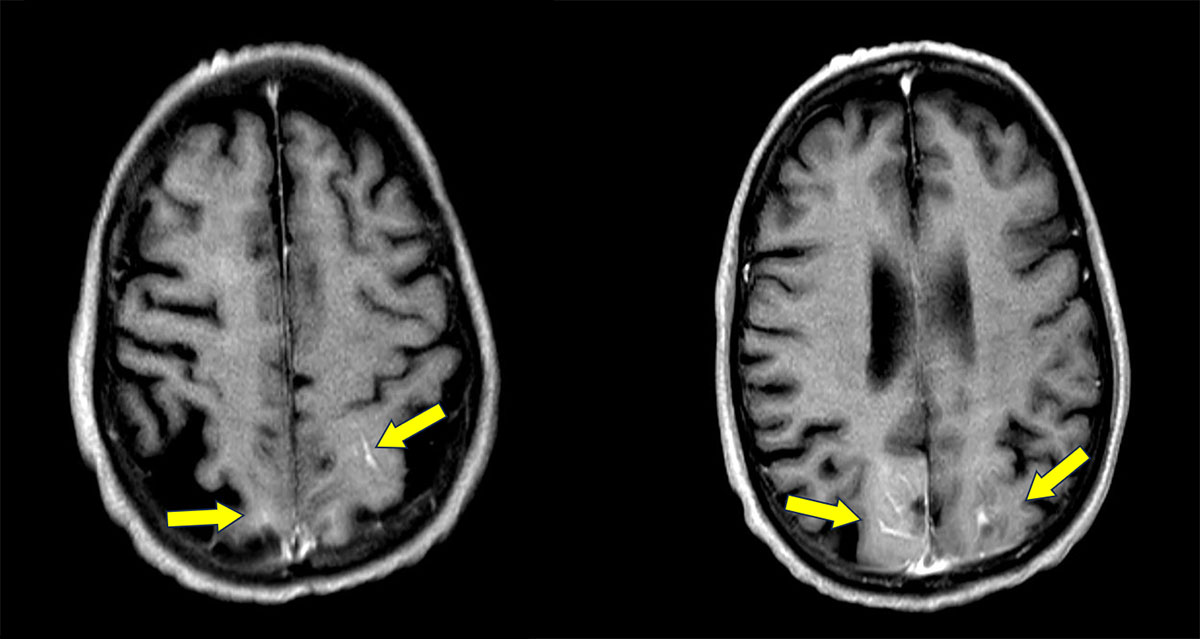
MRI Brain (Day 1):
- FLAIR hyperintensities in the bilateral parietooccipital region.
- Post contrast T1 FLAIR images showing leptomeningeal enhancement in the same areas.
MRI Brain (Follow Up):
Resolution of previously seen FLAIR hyperintensities and leptomeningeal enhancement in bilateral parietooccipital region.
Diagnosis: Cerebral Air Embolism
Discussion
Background:
- Systemic air embolism (SAE) is an extremely rare complication of a CT-guided PTNB, but one that is potentially fatal.
- Reported Incidence: 0.02 to 0.07% (likely underdiagnosed).
- This case highlights the CT and MRI findings of cerebral air embolism post CT guided lung biopsy.
Pathology:
Cerebral air embolism occurs when intravascular air, introduced during procedures such as CT-guided lung biopsy, reaches the cerebral circulation, mechanically obstructs small vessels, triggers endothelial injury and inflammation, and results in acute cerebral ischemia and infarction.
Clinical Presentation:
- Patient can present with sudden neurological deficit (hemiparesis, aphasia, visual loss, or altered sensorium) within minutes.
- They can also present with seizures or cardiopulmonary symptoms (chest pain, dyspnea, arrhythmia, or hypotension)
- The symptoms can be transient or fluctuating and deficits may improve as air redistributes or dissolves.
Diagnosis:
Air embolism is diagnosed by correlating sudden clinical deterioration after procedures such as CT-guided lung biopsy with imaging evidence of intravascular air on CT or MRI, often supported by diffusion-restricted ischemic lesions in the brain.
Neuro-imaging Features:
CT Brain:
- Linear or punctate air foci within cortical sulci or cerebral vessels.
- Air outlining cortical arteries or dural venous sinuses.
- Early scans may be normal if air has dissolved.
- Delayed hypodensity in affected territories due to infarction.
MRI Brain:
- DWI shows acute diffusion restriction in cortical or subcortical regions.
- Lesions often do not follow a single vascular territory.
- SWI or GRE may show blooming from residual intravascular air.
- FLAIR shows cortical sulcal hyperintensity and edema.
- Post-contrast images may show leptomeningeal enhancement.
Treatment:
- It is crucial for radiologists to diagnose cerebral air embolism both during and after lung biopsy, since the patient is usually in the radiology department at the time of symptom onset, and may even still be on the CT table.
- Starting 100 % oxygen immediately can help reduce air bubble size and improves tissue oxygenation.
- Placing the patient supine or in left lateral decubitus position limits further cerebral air migration.
- Starting hyperbaric oxygen therapy as early as possible, this is the definitive treatment and improves neurological outcome.
- Maintain hemodynamic stability, use IV fluids and vasopressors if needed.
- Avoid further air entry, secure lines and stop the procedure at once.
In our case we were able to save the patient due to prompt diagnosis and timely intervention.
References
- Vincent M. Timpone, Andrew L Callen. Characteristic MR Imaging Findings of Cerebral Air Embolism Infarcts: A Case Series American Journal of Neuroradiology May 2024, ajnr.A8349; DOI: 10.3174/ajnr.A8349
- Brown AE, Rabinstein AA, Braksick SA. Clinical Characteristics, Imaging Findings, and Outcomes of Cerebral Air Embolism. Neurocrit Care 2023;38:158- 164
- Kuo HL, Cheng L, Chung TJ. Systemic air embolism detected during percutaneous transthoracic needle biopsy: report of two cases and a proposal for a rountine postprocedure computed tomography scan of the aorto-cardiac region. Clin imaging 2010;34:53-6.
Add a Comment
You must be logged in to post a comment