
May 2022
CASE HISTORY:
A 5month old male child born out of by non-consanguineous marriage presented with history of left focal seizure, reddish discoloration of left hand and delayed attainment of milestones. Parents also noticed increase in fairness of the baby and loss of hair.upper and lower limbs.
Case contributed by –
Dr. Reshma Varghese1, Dr. Lokesh Saini2. Dr Taruna Yadav1 , Dr. Sarbesh Tiwari1
Department of Diagnosis and Interventional Radiology (1) and Department of Pediatrics (2)
All India Institute of Medical Sciences, Jodhpur
 |  |  |  |
 |  |  |
 |  |  |  |
 |  |  | |
Annotations
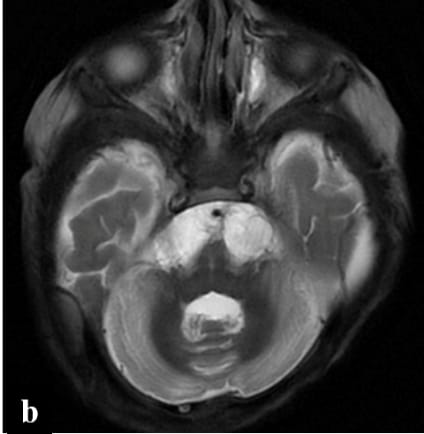
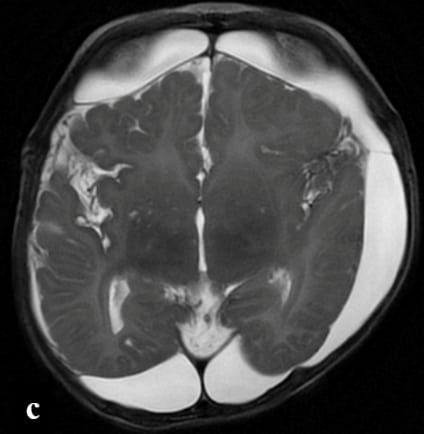
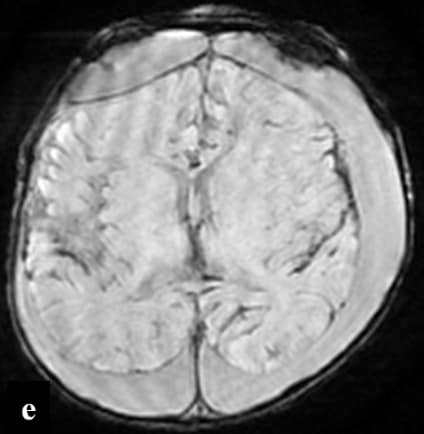
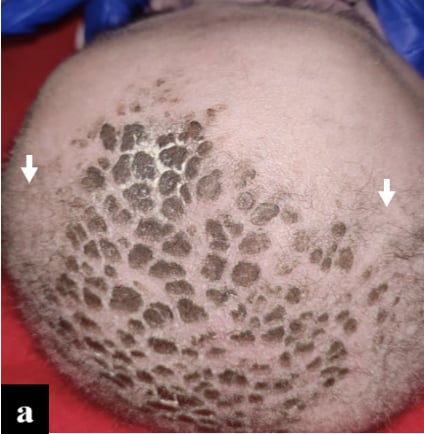
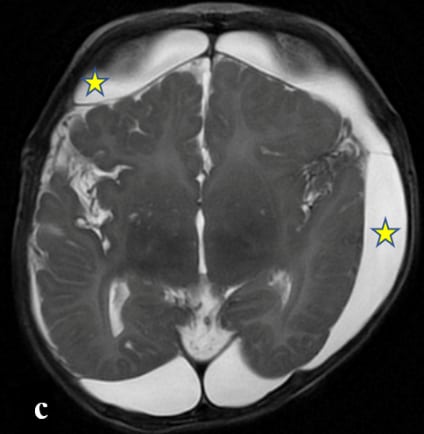
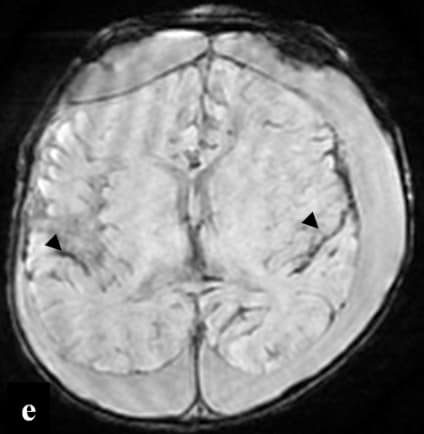
Figure : Image (a) The clinical images of the patient’s scalp shows fair complexion of the child with hypopigmented , sparse and short scalp hair (white arrows). The axial T2 (b & c) images shows bilateral subdural hygroma (asterix) with significant cerebral and cerebellar volume loss. The axial T1 image (d) shows delayed myelination , corresponding to birth. The axial susceptibility weighted images (e & f) shows extensive superficial siderosis along the cerebral sulcal and cerebellar folial spaces (black arrowheads). The time of flight MR angiogram image (g) shows tortuous intracranial and extracranial arteries (dashed arrows).
•Metabolic work up revealed low serum copper and ceruloplasmin levels.
FINAL DIAGNOSIS :Menkes disease (MD)
DISCUSSION:
•Menkes disease (MD) is a rare lethal X-linked recessive disorder due to mutations in the ATP7A gene with incidence of 1 in 300 000 (1), causing impaired absorption and cellular metabolism of copper. Reduced activity of copper-dependent enzymes leads to abnormalities in connective tissue, blood vessels, and hair.
•MRI is the investigation of choice. Cerebral and cerebellar atrophy and delayed myelination are the earliest changes seen (2). Subdural collections are relatively common finding in all children with MDs (3). Basal ganglia can also be involved in Menkes disease, most vulnerable parts are the head of the caudate nucleus and anterior putamen followed by the globus pallidus and it is due to occlusion of small perforating arteries (4).Tumefactive lesions can also be seen, predominantly in temporal lobes which can be symmetric/asymmetric (4). Tortuosity of intracranial vessel is a typical diagnostic feature of Menkes disease (3). Stenosis and ectasia of intracranial vessels are not reported.
References
1.Tümer Z, Møller LB. Menkes disease. Eur J Hum Genet. 2010 May;18(5):511–8.
2.Bindu PS, Taly AB, Kothari S, Christopher R, Gayathri N, Sinha S, et al. Electro-clinical features and magnetic resonance imaging correlates in Menkes disease. Brain and Development. 2013 May 1;35(5):398–405.
3.Manara R, D’Agata L, Rocco MC, Cusmai R, Freri E, Pinelli L, et al. Neuroimaging Changes in Menkes Disease, Part 1. American Journal of Neuroradiology. 2017 Oct 1;38(10):1850–7.
4.Manara R, Rocco MC, D’agata L, Cusmai R, Freri E, Giordano L, et al. Neuroimaging Changes in Menkes Disease, Part 2. American Journal of Neuroradiology. 2017 Oct 1;38(10):1858–65.
Minke kinke disease
Menkes kinky hair syndrome
T1 hyperintensity in Basal ganglia, Vertebrobasilar dolichoectasia and Bilateral chronic subdural hematomas
Menke’s kinky hair disease
Menkes kinky hair disease