
March 2022
CASE HISTORY:
• 23-year female patient presented with history of right sided headache since 1-year with recent onset giddiness and occasional vomiting for 2 months. She has right eye vision loss since birth.
• Neurological examination was normal, except perception of light positivity in right eye
Case contributed by –
• Dr. Priyanka Priyadarshini Baishya– Senior Resident
• Dept Of Neuroimaging and Interventional Radiology, NIMHANS Bengaluru.
• Dr. Jitender Saini –Professor
• Dept Of Neuroimaging and Interventional Radiology, NIMHANS Bengaluru.
 |  |  |  |
 |  |  |  |
 |  |  |  |
 |  |  |  |
 |  |  |  |
 |  |  |  |
LEGENDS:
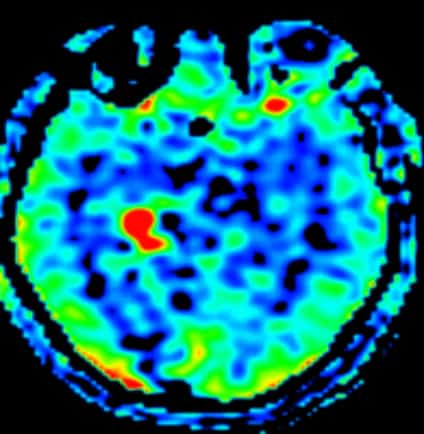
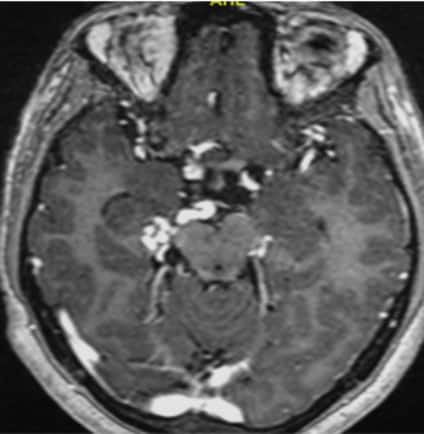
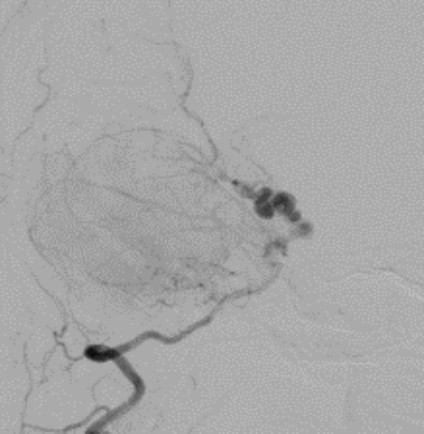
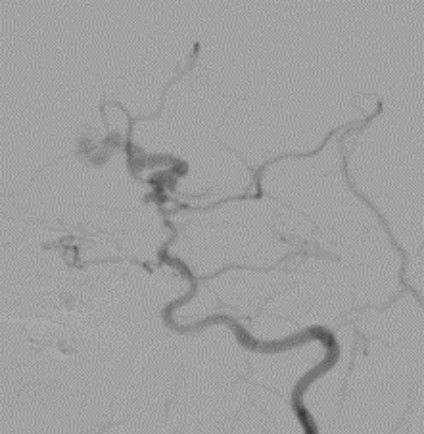
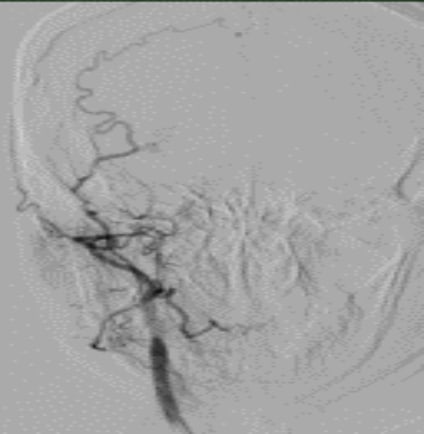
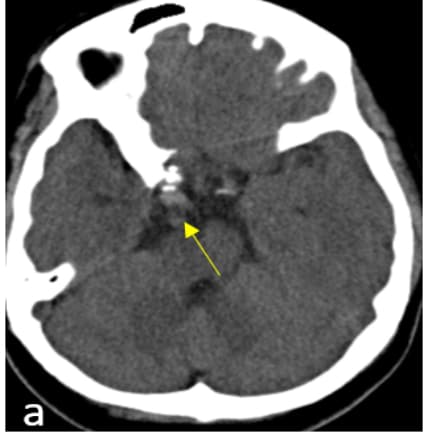
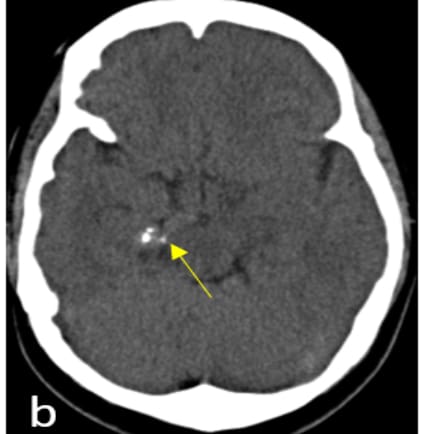
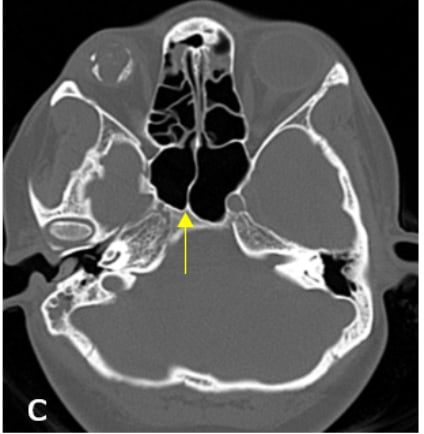
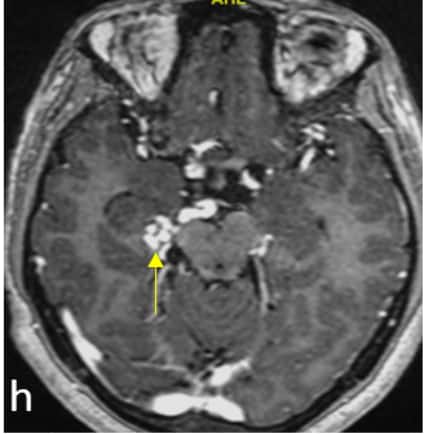
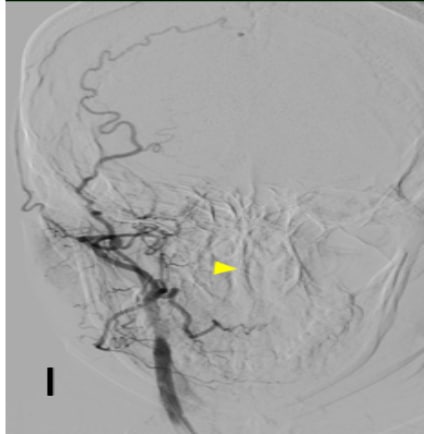
•Axial CT image (a, b) shows hyperdense structures with calcification in the right ambient cistern, bone reformats (c, d) shows hypoplasia and malformed right carotid canal. Calcifications were seen in the shrunken right globe. •Axial T2 weighted images (e, f) shows multilobulated T2 hypointense structures in the right ambient cistern with absence of right ICA flow void. There is right phthisis bulbi. ASL image (g) shows spin trapping in these structures. Post contrast T1 MPRAGE (h) shows lobulated enhancing vessels •DSA image (i, j) reveals ectatic dilated right P1 with multilobulated aneurysmal appearance. There is reformation of the right ACA and MCA from the contralateral circulation through the ACOM. Right PCOM is not visualized ( image k). There is occlusion of right ICA (image l)
Dolichoectasia of right PCA with right ICA occlusion
•Dolichoectasia of the PCA is rarity and is usually postulated to be developmental/ acquired at birth, in contrast to the commoner vertebro-basilar dolichoectasia which is essentially atherosclerotic 1
•Relating to the embryological basis of segmental ICA genesis, this selective vulnerability of the ICA and PCA can be explained by the fact that PCOM and PCA are derived from the caudal ramus of the ICA and are then transferred to the posterior circulation 2,3 .
•Patients can present with non-specific specific symptoms like headache, cranial nerve compression, subarachnoid hemorrhage, transient ischemic attacks or infarcts and management varies accordingly- medical management to surgery/ intervention
•Imaging- CT, CTA, MRI and MRA plays a crucial role in diagnosis and DSA being able to demonstrate the vascular nature of the lesion and facilitate appropriate management.
•Learning point: Affliction of ICA and PCA in this case can be explained by segmental vulnerability due to vascular insult/ infection in the perinatal / in utero period causing mutilation of the endothelium, leading to ICA occlusion and dolichoectasia of PCA.
References:
1. Pico F, Labreuche J, Amarenco P. Pathophysiology, presentation, prognosis, and management of intracranial arterial dolichoectasia. Lancet Neurol. 2015 Aug;14(8):833–45.
2. Lasjaunias PL. Segmental Identity and Vulnerability in Cerebral Arteries. Interv Neuroradiol. 2000 Jun;6(2):113–24.
3. Kobkitsuksakul C, Somboonnitiphol K, Apirakkan M, Lueangapapong P, Chanthanaphak E. Dolichoectasia of the internal carotid artery terminus, posterior communicating artery, and posterior cerebral artery: The embryonic caudal ramus internal carotid segmental vulnerability legacy. Interv Neuroradiol. 2020 Apr;26(2):124–30.
PHACES syndrome