
July 2021
Interesting case of headache
•56 female
•Acute onset severe headache – holocranial- thunderclap type while bathing with no postural variation. Recurrent vomiting and neck stiffness.
•Prior H/o disabling migraine attacks
•CSF – Blood stained with near normal protein levels and normal sugar levels.
•Vasculitis profile – negative
•Initial CT and MR angio- normal. Prior Imaging of spine showed suspected spinal SAH and leptomeningeal enhancement
•Review MRI, MR angio and DSA done
Case contributed by –
1.Dr Arun Prasad B, Senior resident, Dept of IS & IR, SCTIMST
2.Dr Sachin Girdhar, Senior resident, Dept of IS & IR, SCTIMST
3.Dr Dev Prakash Sharma, Senior resident, Dept of IS & IR, SCTIMST
4.Dr C Kesavadas, Professor, Dept of IS & IR, SCTIMST
 |  |  |
 |  |  |
 |  |  |  |
 |  |  |  |
 |  |
 |  |  |  |
 |  |
 |  |  |  |
 |  |  |  |
 |  |
 |  |  |  | |
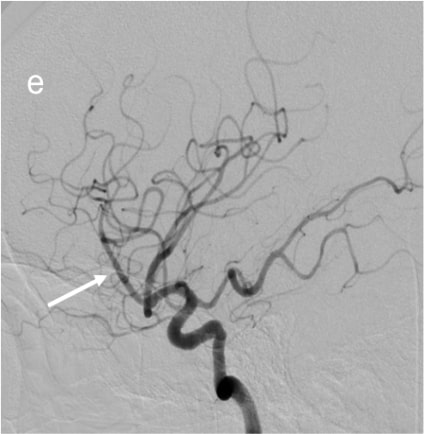 | 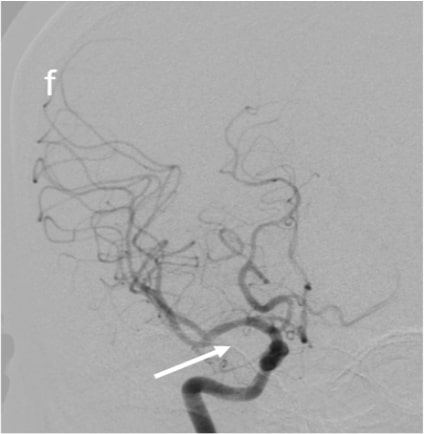 | 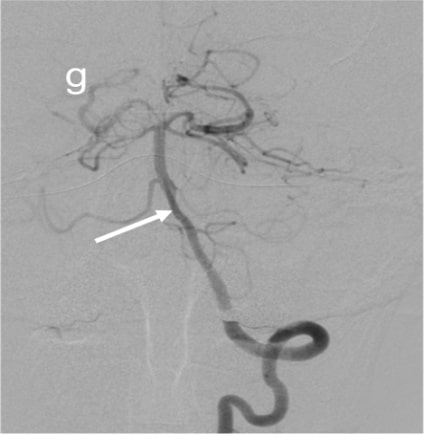 | 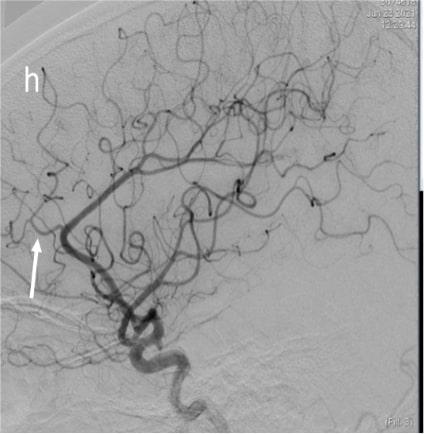 |  |
Figure Legends
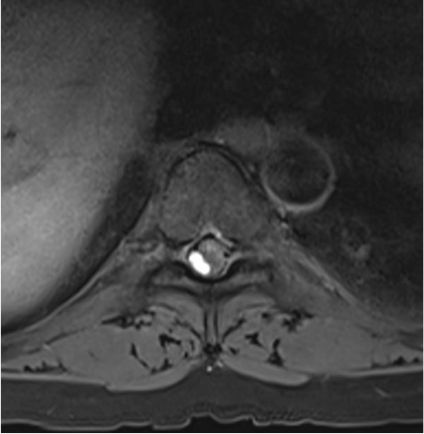
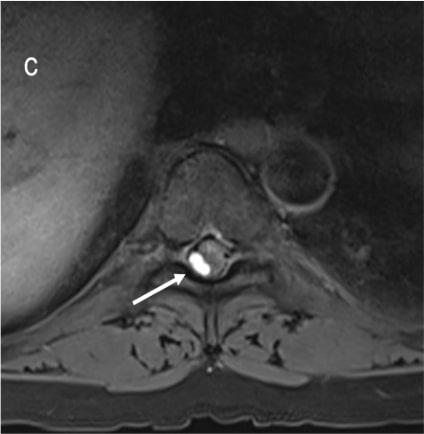
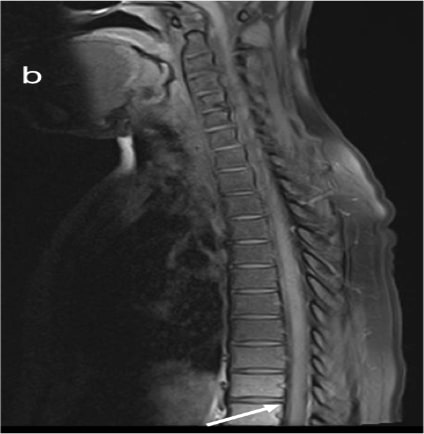
Figure 1 (a & c) :
Axial T2WI and Pre contrast Axial T1FS images showing hyperintense right posterolateral spinal subdural hematoma in dorsal spine(indicated by white arrows); Figure1 (b&d) Axial T2WI and Pre contrast Axial T1FS images showing spinal SAH/SDH at lumbosacral spine(indicated by white arrows). Figure1(e&f), Sagittal Pre T1FS of dorsolumbar spine and sagittal gradient images of lumbosacral spine showing hyperintense SDH with minimal hemosiderin staining on gradient images indicated by white arrows)
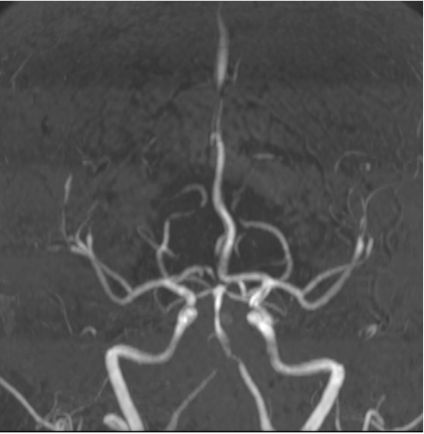
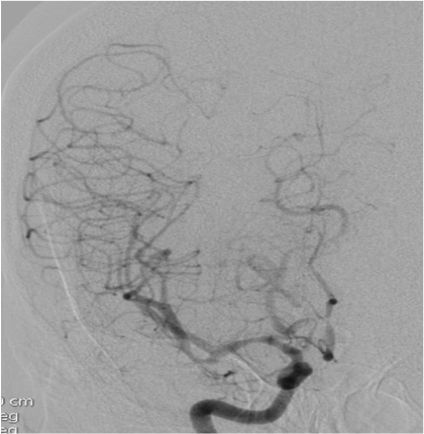
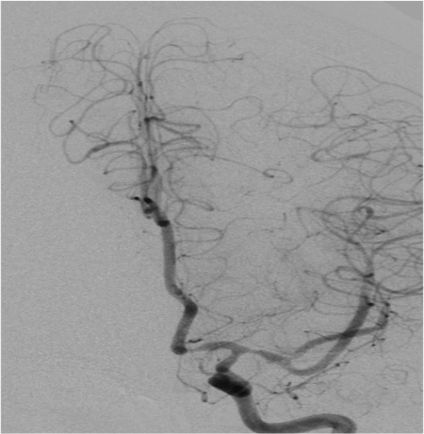
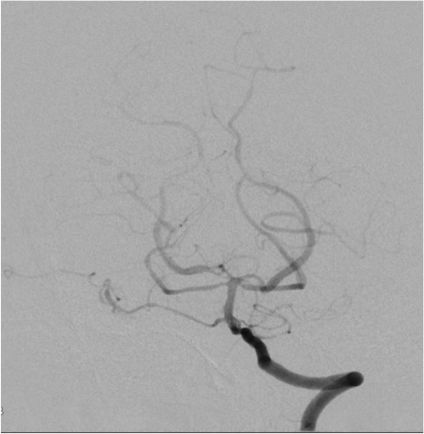
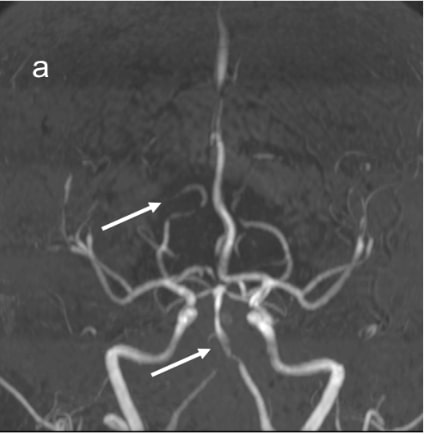
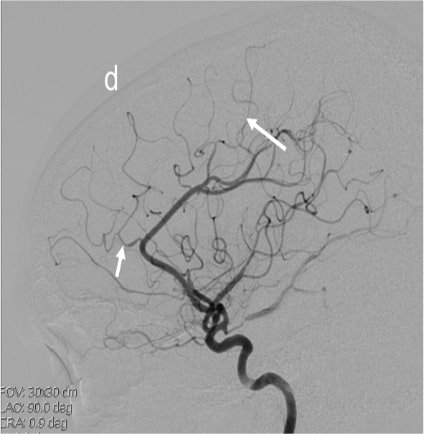
Figure 2 (a & b):
Anteroposterior and sagittal MIP reformats of the 3D TOF MRA showing focal stenosis of basilar formation, distal basilar artery and right P3 PCA (Indicated by white arrows). Figures 2(c&d) Anteroposterior and sagittal DSA images of left ICA injection showing focal stenosis of left A1ACA, M1MCA & M2MCA(a) and focal stenosis of left A3 ACA and A4ACA distal branches(indicated by white arrows); Figure 2 (e&f) Anteroposterior and sagittal DSA images of right ICA injection showing focal stenosis of right A1ACA and M1MCA(e) and focal stenosis of right A3 ACA and A4ACA distal branches(indicated by white arrows); Figure2(g&h) Sagittal and Anteroposterior DSA images of left vertebral artery injection showing Irregularity and narrowing of distal P3 branches(g&h) and also irregularity and narrowing of basilar artery (h) (indicated by white arrows).
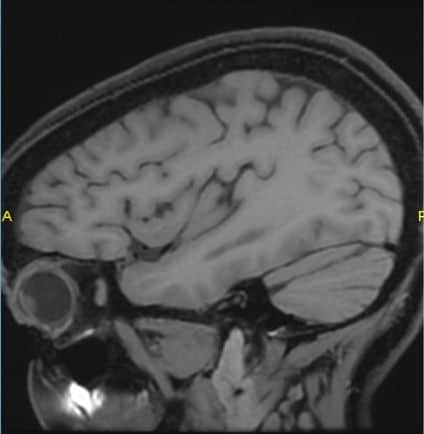
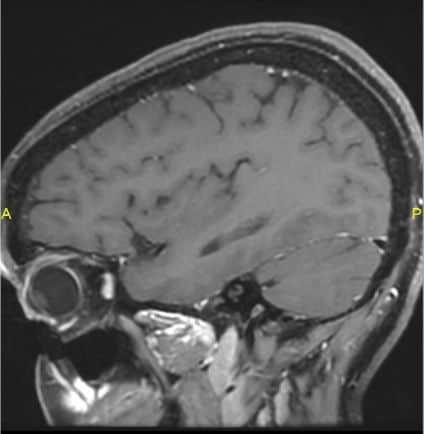
Figure 3(a & b) :
Sagittal 3D CUBE pre and post contrast FS images showing concentric mild wall thickening and minimal enhancement of the superior division of left M1MCA (indicated by white arrows).
Figure 4 (a & b) :
Axial and sagittal T1FS images of cervicodorsal spine showing resolution of the subdural hematoma at D7 level(indicated by white arrows). Figure 4(c&d)Sagittal T2 Cervical and Lumbosacral spine showing resolution of the SDH.Figure4(e&f) showing right ICA AP and LAT injections showing resolution of the focal stenosis in the locations mentioned in figure 2. Figure 4(g) showing resolution of basilar artery focal stenosis. Figure4(h&i) showing resolution of focal stenosis of right A1ACA and M1MCA and focal stenosis of right A3 ACA and A4ACA distal branches(indicated by white arrows).
•Final diagnosis : Acute spontaneous spinal subdural hematoma with multifocal intracranial vasospasm/Reversible cerebral vasoconstriction syndrome(RCVS).
•Intracranial subdural hemorrhage or subarachnoid hemorrhage are known associated entities with RCVS. However, association of RCVS with acute spontaneous spinal subdural hematoma is very rare.(1,2)
•This is a very peculiar case where the patient did not present with any spinal symptoms and had only thunderclap headache.
•Hypothesis :Occurrence of spontaneous spinal subdural hematoma after a subarachnoid bleed due to sudden raised intrathoracic pressure à Trigger factor for development of intracerebral vasoconstriction syndrome.(1)
•RCVS can be differentiated from CNS vasculitis by vessel wall MRI which shows vessel wall thickening with minimal or no enhancement (4). Certain studies have also shown that RCVS is more likely to be associated with subarachnoid hemorrhage, superficial lesions, sausage appearance of vessels in angiography.(5)
•Hence whether the RCVS is a causative factor or an associated factor of acute spontaneous spinal subdural hematoma is still not clear. This may be due to the extreme rarity of this condition coupled with lack of literature evidence.(2,3)
References
1. Oh, Jung-Hwan & Jwa, Seung-Joo & Yang, Tae & Oh, Kyungmi & Kang, Ji-Hoon. (2015). Intracranial Vasospasm without Intracranial Hemorrhage due to Acute Spontaneous Spinal Subdural Hematoma. Experimental Neurobiology. 24. 366. doi: 10.5607/en.2015.24.4.366.
2. Santos, Laura*; Azevedo, Elsa Reversible cerebral vasoconstriction syndrome – A narrative revision of the literature, Porto Biomedical Journal: May 2016 – Volume 1 – Issue 2 – p 65-71.doi: 10.1016/j.pbj.2016.04.002.
3. J. Kang, J. Oh, S. Jwa, H. Ma. Intracranial vasospasm associated with acute spontaneous spinal subdural hematoma. Journal of the Neurological Sciences. Volume 357,Supplement 1,2015,Page e385.ISSN 0022-510X,https://doi.org/10.1016/j.jns.2015.08.1369.
4. Mandell DM, Matouk CC, Farb RI, Krings T, Agid R, terBrugge K, Willinsky RA, Swartz RH, Silver FL, Mikulis DJ. Vessel wall MRI to differentiate between reversible cerebral vasoconstriction syndrome and central nervous system vasculitis: preliminary results. Stroke. 2012 Mar;43(3):860-2. doi: 10.1161/STROKEAHA.111.626184.
5. Saygin D, Cerejo R, Sundaram-Simonelli P, Toth G, Jones S, Calabrese LH, Hajj-Ali RA. Differentiating Features of Primary Angiitis of Central Nervous System and Reversible Cerebral Vasoconstriction Syndrome: Clinical and Radiological Evaluation [abstract]. Arthritis Rheumatol. 2017; 69 (suppl 10)
Spontaneous spinal subarachnoid hemorrhage.
RCVS with Spinal SAH