
Dec 2022
CASE HISTORY:
39 years , male, presented with progressive gait disturbance and speech difficulty since 11 months. Associated with headache, giddiness and vomiting since 3-4 months.
CASE CONTRIBUTED BY
Department of Diagnostic and Interventional Radiology, AIIMS Jodhpur
 |  |  |  |  |
 |  |  |  |
 |  |  |  |
 |  |  |  |
 |
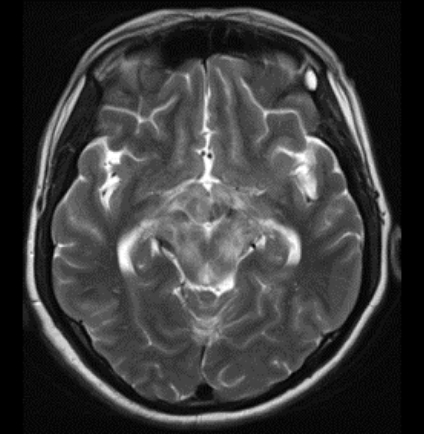
Image A & B – Axial T2 weighted images at the level midbrain and pons respectively shows ill defined T2 hypointense lesion with associated edema causing diffuse expansion of the brainstem.
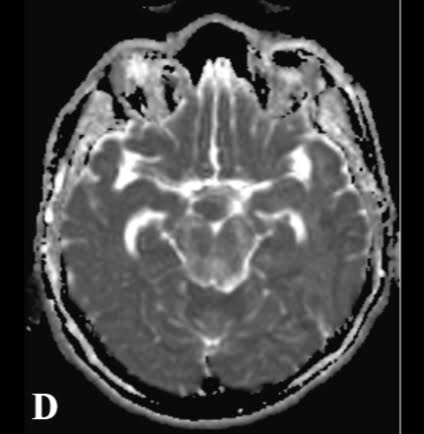
Image C & D – The trace and ADC images of Diffusion weighted imaging shows patchy areas of restricted diffusion.
Image E – T2 sagittal images shows diffusion involvement of the brainstem and the hypothalamic region ( black arrow).
Image F-H : The post contrast T1MPRAGE images shows ill defined nodular enhancing lesions in random distribution in brainstem, hypothalamus and the superior vermis.
Image I : Multiple ill defined small thin walled variable shaped cysts seen distributed throughout all lobes in both lungs along with interstitial septal thickening.
Discussion
•Erdheim-Chester disease (ECD) is a rare non–Langerhans cell histiocytosis. Typically affects middle-aged patients and is slightly more common in men (1).
•Multiple somatic mutations are implicated in ECD, most commonly BRAF V600E.
•ECD is a multisystem disorder commonly involving perinephric fat (68%), the periaortic region (66%), lungs (43%), pericardium (42%), orbits (25%), and the neuroaxis (51%); 25% have diabetes insipidus (DI) (2).
•C/F :
•Diabetes insipidus- secondary to involvement of the hypothalamic-pituitary axis (HPA)
•Ataxia – owing to involvement of posterior fossa structures, particularly the cerebellar dentate nuclei (3).
•Exophthalmos, retroorbital pain, extraocular muscle palsies, and progressive vision loss – Orbits are involved in 1/4th of patients/
•Additional common symptoms include bone pain, weakness and fatigue, cough and progressive respiratory failure, ureteral obstruction, renal impairment, cardiac dysfunction and tamponade, and xanthelasmas and xanthomas.
Discussion: Key Diagnostic Features:
•Intracranial disease may be intra-axial and/or extra-axial and is commonly multifocal.
•Extra-axial lesions may present as a plaque like thickening of dura.
•Intra-axial lesions are often FLAIR hyperintense with predilection for the pons, brachium pontis and the hypothalamic pituitary axis.
•Avid postcontrast enhancement is typical. Both diffuse and nodular enhancement is possible.
•CNS findings are generally nonspecific, but the additional findings of sclerotic bone lesions and pericardial, pulmonary interstitial, and retroperitoneal infiltrative soft tissue thickening should raise suspicion for this disease (3).
References
•1. Verdalles U, Goicoechea M, García de Vinuesa S et-al. Erdheim-Chester disease: a rare cause of renal failure. Nephrol. Dial. Transplant. 2007;22 (6): 1776-7.
•2. Myra C, Sloper L, Tighe PJ et-al. Treatment of Erdheim-Chester disease with cladribine: a rational approach. Br J Ophthalmol. 2004;88 (6): 844-7.
•3. Johnson MD, Aulino JP, Jagasia M et-al. Erdheim-chester disease mimicking multiple meningiomas syndrome. AJNR Am J Neuroradiol. 2004;25 (1): 134-7.
Add a Comment
You must be logged in to post a comment