
Dec 2022
CASE HISTORY:
A 31 year old male presented with history of seizures since 2 months. He was treated with anti epileptics and was well controlled. Patient again developed breakthrough seizures. No focal neurological deficits.
Auto immune work up & CSF analysis were unremarkable.
MRI Brain (Plain & Contrast) were performed.
CASE CONTRIBUTED BY
Dr Sumana Kedilaya, Registrar, Department of Radiology, Apollo Sheshadripuram Bangalore
Dr Vikram Kamat, Senior consultant Neurologist, Trustwell Hospital, Bangalore
Dr Chaitra Adiga, Consultant, Department of Radiology, Apollo Sheshadripuram Bangalore
 |  |  |  |  |
 |  |  |  |  |
 |
Initial MRI
 |  |  |  |
 |  |  |  |
 |  |  |
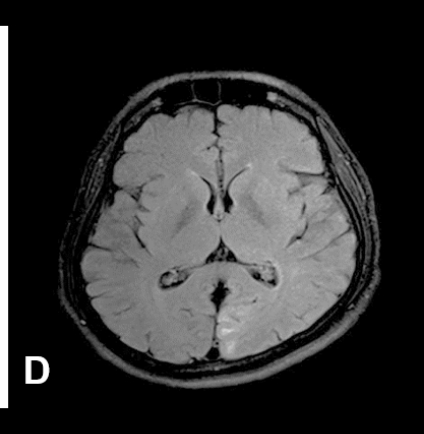
ØFig A-D (initially performed MRI) shows predominantly cortical T2W/FLAIR hyperintensity in left parasagittal parieto-occipital lobes. No true restricted diffusion or bleed noted.
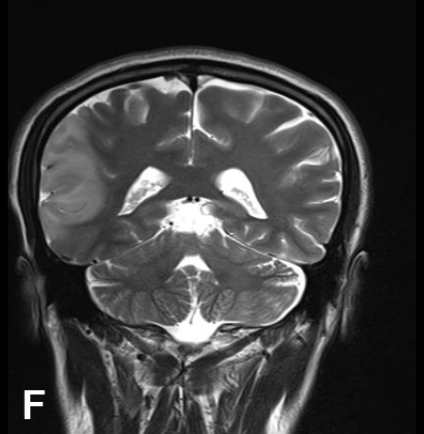
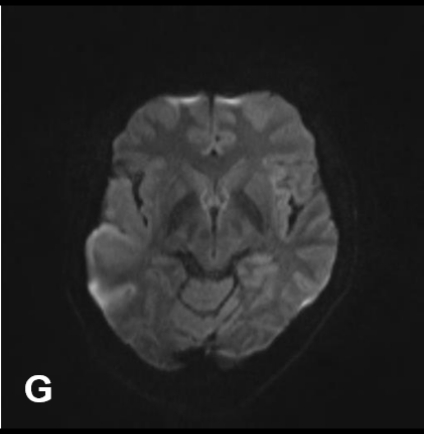
Ø(Repeat MRI after 3 months) Fig E-I show T2W/FLAIR hyperintensity with high signal intensity on DWI & ADC representing T2-Shine through in the right parieto-temporal cortex & subcortical white matter
ØFig J (post contrast administration) did not reveal significant enhancement.
ØFig K (MRS) showed elevated lactate is noted.
FINAL DIAGNOSIS:
ØMELAS (Mitochondrial Encephalomyopathy with Lactic Acidosis and Stroke like Episodes)
BACKGROUND:
ØMELAS is a rare mitochondrial metabolic disease, and affected patients have maternal pattern of inheritance.
Ø>80% of MELAS cases are due to point mutation in nucleotide 3243 mtDNA (A to G translocation) in MT-TL1 gene which codes for t-RNA(1)
ØtRNA mutations lead to the absence or deficit of subunits of the respiratory chain protein complexes, can lead to impaired function of cells/their death.
CLINICAL FEATURES:
ØOnset of MELAS is typically during childhood between 2 -20 years, although it can get delayed until between 10-40 years
ØPresent with symptoms such as stroke like episodes, seizures, recurrent headaches, failure to thrive, developmental delay, sensorineural hearing loss, lactic acidosis, cortical blindness(2)
IMAGING FEATURES:
ØStroke Like episodes are probably caused by abnormal mitochondria in the endothelial and smooth muscle cells of blood vessels, leading to impairment of the autoregulatory vascular mechanisms.
ØMust be differentiated from ischemic vascular strokes because different management is required
ØMELAS lesions are mostly in posterior & lateral brain regions (parieto occipital lobes & temporal lobes)
ØMigratory T2W hyperintense lesions involving cortex & subcortical white matter(3)
ØHigh signal intensity on DWI with varying intensity on ADC map which reflects cytotoxic/ vasogenic edema (3)
ØMRS typically shows elevated lactate and reduced NAA, glutamate, myo-inositol and total creatine.
ØNo reduction in regional cerebral blood flow in the affected areas in MELAS (2)
ØCerebral angiography most commonly reveals normal findings (1)
References
1.Primary Mitochondrial Disorders of the Pediatric Central Nervous System: Neuroimaging Findings Fabrício Guimarães Gonçalves, César Augusto Pinheiro Ferreira Alves, Beth Heuer, James Peterson, Angela N. Viaene, Sara Reis Teixeira, Juan Sebastián Martín-Saavedra, Savvas Andronikou, Amy Goldstein, and Arastoo Vossough RadioGraphics 2020 40:7, 2042-2067
2.Pauli W, Zarzycki A, Krzyształowski A, Walecka A. CT and MRI imaging of the brain in MELAS syndrome. Pol J Radiol. 2013 Jul;78(3):61-5. doi: 10.12659/PJR.884010. PMID: 24115962; PMCID: PMC3789935.
3.Cheng W, Zhang Y and He L (2022) MRI Features of Stroke-Like Episodes in Mitochondrial Encephalomyopathy With Lactic Acidosis and Stroke-Like Episodes. Front. Neurol. 13:843386.
Add a Comment
You must be logged in to post a comment