
Aug 2022
CASE HISTORY:
A 36 year old hypertensive male presented with gradually progressive weakness of bilateral upper and lower limb weakness since 1-2 months. Preliminary MRI was performed following which CT angiography was advised on account of suspicion of vascular malformation.
Case contributed by –
Dr Sabha Ahmed
Senior Resident
Department of Neuroimaging and Interventional Radiology, NIMHANS Bangalore
Dr Ankit Arora
Senior Resident
Department of Neuroimaging and Interventional Radiology, NIMHANS Bangalore
Dr Jitender Saini
Professor
Department of Neuroimaging and Interventional Radiology, NIMHANS Bangalore
 |  |  |  |
 |  |  |
 |  |  |
Figure B and C: The lesion appears heterogeneous signal intensity on Sagittal T1 and shows mild post contrast enhancement.
Suspecting a vascular lesion, CT Angiography was planned for the patient.
 |  |  |  |
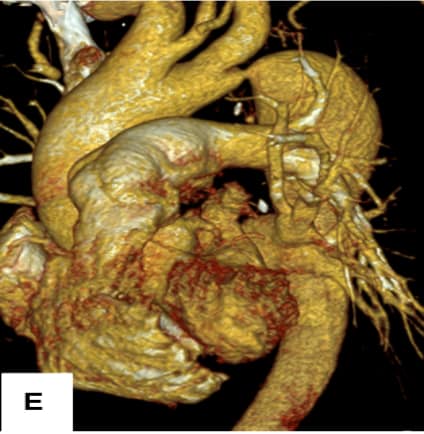
Common origin of Brachiocephalic trunk and left CCA was noted (Arrows).
Figure F: Coronal MIP reformats demonstrate a saccular aneurysm in the spinal canal,at the hairpin bend of anterior spinal artery (Arrow). Note the presence multiple tortuous paravertebral collaterals.
Figure G: Sagittal MIP reconstructions show the saccular aneurysm (Arrow), posterior to C6 vertebral body corresponding to the hypointense lesion on MRI causing cord compression.
ANTERIOR SPINAL ARTERY ANEURYSM
Isolated ASA aneurysms are rare in general, however they can be found in association with arteriovenous malformations of the spine, Moyamoya disease, aortic coarctation,, vasculitides, and rarely infections.(1)
ASA aneurysms are commonly either wide-necked saccular or fusiform and smaller in size with index presentation of bleed or with mass effect on the cord. Any underlying chronic vascular obstruction finds opening of multiple collateral channels develop thereby offering an important alternative source of blood supply when the original vessel fails to meet with the demands of afflicted structure/organ.
The main collaterals in coarctation of aorta are via the internal mammary and the intercostal arteries, in particular -the intercostals and subclavian arterial branches, with additional recruitment from other vessels such as the vertebral, spinal, suprascapular, long thoracic, and epigastric arteries (2).
The ASA acting as a collateral channel is rather rare, but in our case it is involved in the collateral via the left subclavian artery that culminated in the formation of flow related aneurysm pathophysiologically described in association with narrowing of descending thoracic or abdominal aorta and subsequnet altered hemodynamic factors.
The phenomenon of “aortic steal’’ where aorta distal to the obstruction is proposed to be stealing blood from the ASA through the radicular artery, has been previously described in CoA is seen in our cas.
Myelopathy is a seldom reported presenting feature of CoA with propositions of compression due to dilated intraspinal collaterals, subarachnoid hemorrhage or spinal or radicular artery aneurysms.
Compression in a relatively tight spinal canal of the lower cervical and upper thoracic regions, ischemic events or aortic steal that can occur due to microemboli from ectatic collateral channels may further act as a source of a clot (3).
In cases of ruptured ASA aneurysm associated with CoA, a surgical or endovascular treatment of aneurysm with immediate anatomical correction of the disease is said to best prevent subsequent SAH (4).
Our case was treated with surgical clipping of ASA aneurysm.
Clinical Learning Point: ASA aneurysms, although rare, can be found in scenario of chronic vascular obstruction such as Aortic stenosis/coarctation and can present with spinal subarachnoid hemorrhage/compressive myelopathy.
Radiological Learning Point: In patients with coarctation of Aorta , presenting with compressive myelopathy and MRI suggestion of extramedullary T2 hypointensity, should raise the suspicion of ASA aneurysms.
REFERENCES
1. Berlis A, Scheufler KM, Schmahl C, et al. Solitary spinal artery aneurysms as a rare source of spinal subarachnoid hemorrhage: Potential etiology and treatment strategy. AJNR Am J Neuroradiol 2005; 26: 405–410.
2. Sharma S, Kumar S. Hematomyelia due to anterior spinal artery aneurysm in a patient with coarctation of aorta. Neurol India 2010; 58: 675–676
3. Aoun SG, El Ahmadieh TY, Soltanolkotabi M, et al. Ruptured spinal artery aneurysm associated with coarctation of the aorta. World Neurosurg 2014; 81: 441.e17–e22.
4. Singh V, Naik S, Bhoi SK, Phadke RV. Anterior spinal artery aneurysm in aortic stenosis of different etiology: Report of three cases. Neuroradiol J. 2017 Apr;30(2):180-185
Coarctation of aorta with anterior spinal artery aneurysm