
April 2022
CASE HISTORY:
• . Case history
50 year old man presented with history of pyrexia of unknown origin, dull headache ,right ear pain, left side weakness and difficulty in swallowing.
On neurological examination:
Right side diplopia on looking at far objects
Reduced sensation on right side of face
Dysarthria
Motor weakness on left side; 3/5 power on upper and lower limbs.
Case contributed by –
• Dr. Krishnendhu MS, Radiology, Manipal Hospitals, Bangalore.
•Dr. Ullas V Acharya , Radiology, Manipal Hospitals, Bangalore.
•Dr. Manjunath M, Neurology, Manipal Hospitals, Bangalore.
•Dr. Neha Mishra, Infectious diseases, Manipal Hospitals, Bangalore.
 |  |  |  |
 |  |  |  |
 |  |  |  |
 |  |  |  |
Annotations
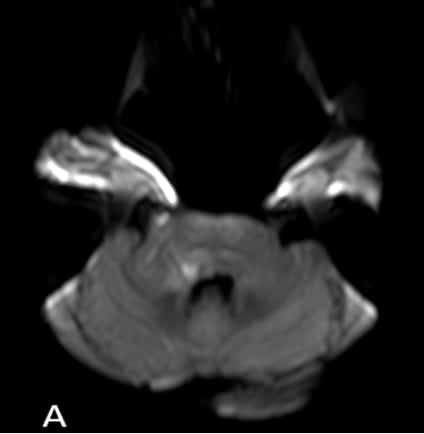
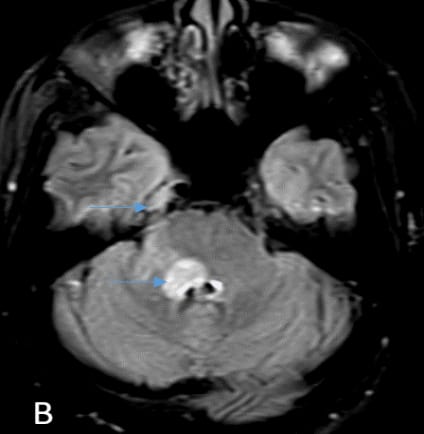
Axial DWI, FLAIR and T2W imaging (A,B,C) shows focal ovoid diffusion restriction in right dorsal pons with linear extension of hyperintense signals across lateral surface of pons and middle cerebellar peduncle.
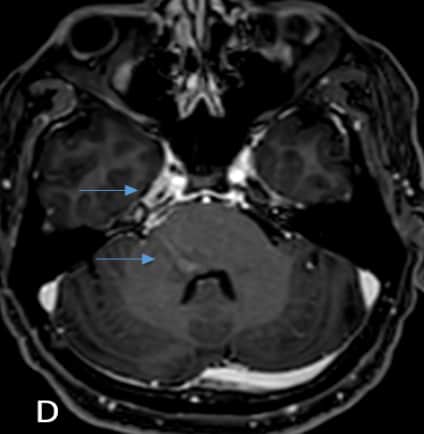
(D) Axial T1W post contrast sequence shows ovoid enhancement of right dorsal pons with linear streak of enhancement along right lateral surface of pons and MCP. Enhancement of trigeminal nerve along the cisternal segment and in Meckel’s cave.
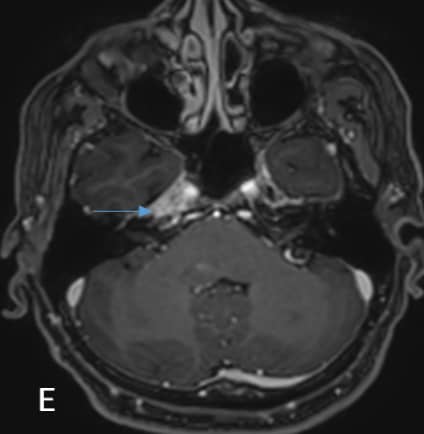
(E) Axial T1W post contrast sequence shows enhancement of right petrous apex.
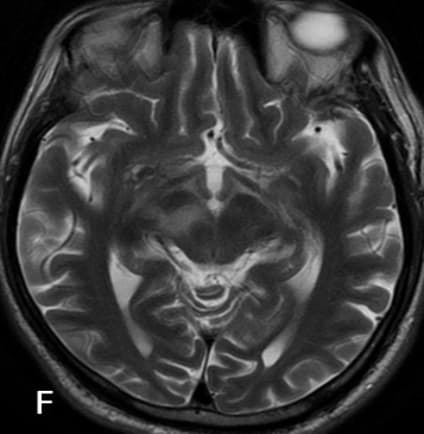
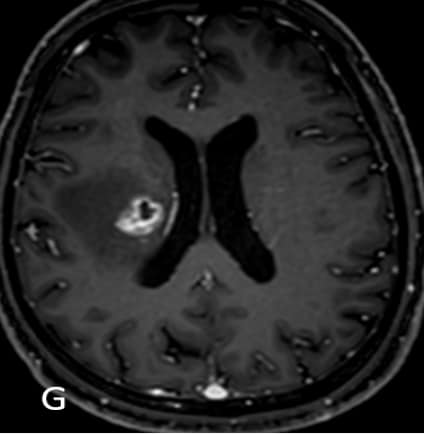
(F) Axial T2W and (G)(H) T1W post contrast images shows ring enhancing lesions in right corona radiata and adjacent basal ganglia with surrounding oedema extending along the corticospinal tracts of the corona radiata, internal capsule, midbrain and cerebral peduncle.
NEUROMELIOIDOSIS
•Melioidosis is an infection caused by the environmental saprophytic gram-negative bacillus Burkholderia pseudomallei.
•Immunocompromised individuals, diabetics and alcoholics are more susceptible.
•Inhalation, ingestion of contaminated material and inoculation through abraded skin are the modes of acquisition. •Neuromelioidosis is rare and associated with higher rates of mortality.
•Spread of microabscesses along white matter tracts including corticospinal tracts, corpus callosum, and cerebellar peduncles along with frequent trigeminal nerve involvement are unique imaging characteristics of CNS melioidosis. These findings provide insight into potential mechanisms for B. pseuodomallei entry into the CNS through direct axonal transport in cranial nerves bypassing the blood brain barrier.
•Involvement of adjacent calvarium (erosions, destruction, marrow edema) and/or scalp (edema or collections) can also be seen in large number of cases.
References:
•Mannam P, Arvind VH, Koshy M, Varghese GM, Alexander M, Elizabeth SM. Neuromelioidosis: A Single-Center Experience with Emphasis on Imaging. Indian J Radiol Imaging. 2021 Jan;31(1):57-64.
•Hsu CC, Singh D, Kwan G, Deuble M, Aquilina C, Korah I, et al. Neuromelioidosis: Craniospinal MRI Findings in Burkholderia pseudomallei Infection. J Neuroimaging. 2016 Jan-Feb;26(1):75-82.
•Hsu CC, Singh D, Kwan G, Deuble M, Aquilina C, Korah I, et al. Neuromelioidosis: Craniospinal MRI Findings in Burkholderia pseudomallei Infection. J Neuroimaging. 2016 Jan;26(1):75-82.
Neuromelidiosis
Neuromalleodosis
Neuromelidiosis
Neuromelidiosis