
Feb 2025
CASE HISTORY
A 11-year-old male child presented with long-standing drug-resistant epilepsy. NCCT head was performed after a seizure episode in the neuro casualty, subsequently MRI brain was performed for further characterization.
CASE CONTRIBUTED BY
Dr. Srinivas Meharwade, Radiology, NIMHANS, Bengaluru
Dr. Gauri Bornak, Radiology, NIMHANS, Bengaluru
Dr. Sabha Ahmed, Radiology, NIMHANS, Bengaluru
CT Brain Findings
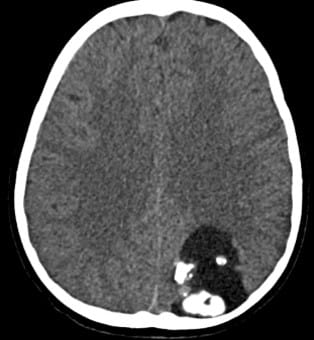
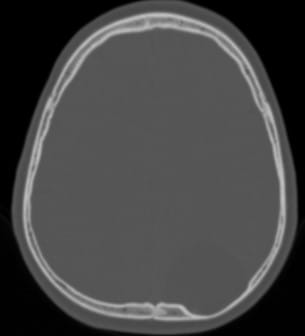
The non contrast CT of the brain shows a well circumscribed mass in the left parietal lobe showing chunky areas of calcifications within (arrows in figure A). The rest of the mass shows predominant fluid attenuation (Hounsfield units not shown). It is causing scalloping of the overlying left parietal bone indicating a slow growing nature of the mass
Location: Left parietal lobe
Features: Well-circumscribed, calcifications (arrows in figure A), fluid attenuation
Bone: Scalloping of left parietal bone
Growth: Indicates slow-growing mass

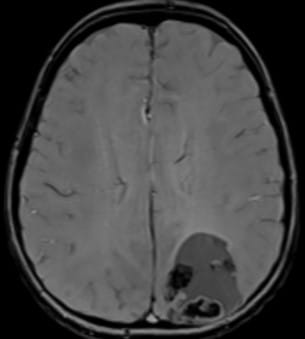
MRI Brain Findings
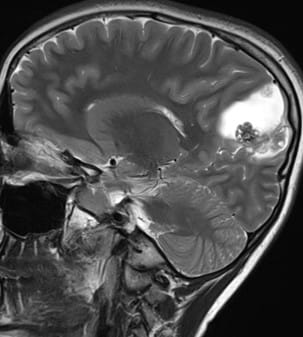
Lesion Location: Left precuneus
Characteristics:
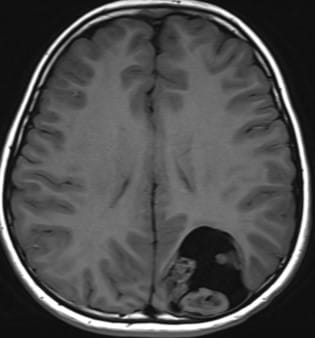
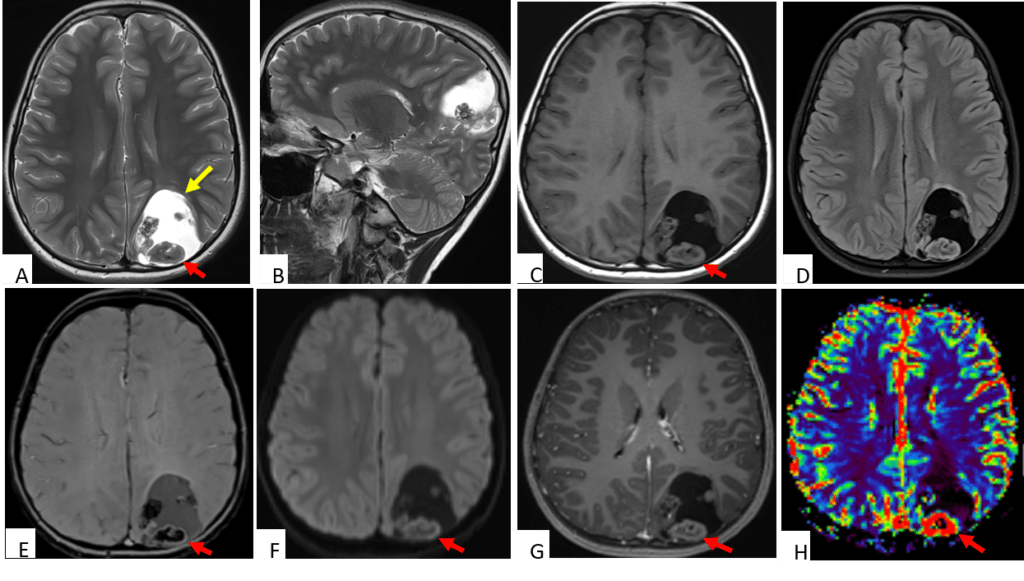
– Well-circumscribed, intra-axial, cortical-based solid-cystic lesion (Fig A & B)
– Multiple T2 hypointense nodules along periphery (red arrow in Fig A)
– Isointense on T1 (Fig C), blooming on SWI (Fig E)
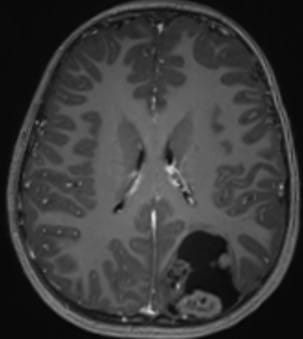
– Mild post-contrast enhancement (Fig G)
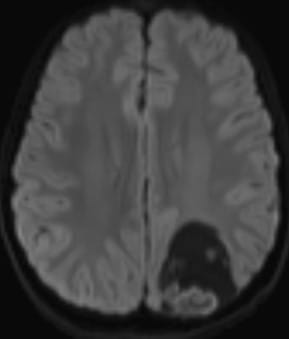
– No significant diffusion restriction (Fig F)
– No rim enhancement
– Complete FLAIR suppression of cystic component (Fig D)
– No perilesional vasogenic edema
– Elevated perfusion values in solid nodules on rCBV maps (Fig H)
– The patient underwent left parietal craniotomy and excision of the lesion.
– The histopathology report revealed relatively circumscribed moderately cellular glial tumour with cells arranged in sheets and perivascular pattern. Extensive dystrophic calcification with stromal proliferating thin walled blood vessels, areas of hemorrhage were seen.
– Immunohistochemistry revealed positivity for OLIG2, GFAP, CD34. In addition, it showed IDH1p.R132H negativity, retained ATRX expression and was negative for p53
 |  |  |  |
 |  |  |  |
Diagnosis
Polymorphous Low-grade Neuroepithelial Tumour of the Young (PLNTY)
Polymorphous Low-Grade Neuroepithelial Tumor of the Young (PLNTY)
Background
- Newly classified in the 2021 WHO brain tumor classification
- Categorized under pediatric-type low-grade diffuse gliomas
- First described in 2017
- Non-neuronal and non-ependymal subtype
- Associated with long-term epilepsy
Clinical Presentations
- Typically affects children and young adults (median age: 17.5 years)
- No gender predilection
- Commonly causes early-onset epilepsy, often resistant to antiepileptics
- May present with headaches or be an incidental finding
Pathology
Histopathologic analysis shows:
- Calcifications
- Intense CD34 immunoreactivity (differentiates from oligodendroglioma)
- Mutually exclusive BRAF mutations or FGFR2/3 fusions (activates MAP kinase pathway)
Imaging features
- PLNTY are typically cortical based lesions and show hyperintense or mixed density on T2 and hypointense on T1 imaging with frequent macroscopic calcifications. They show variable post contrast enhancement.
- The lesion may show peripheral cystic components.
- Temporal lobe location (although lesions have been reported in parietal, frontal, and occipital lobes).
Differential Diagnosis
- The differential diagnosis mainly includes other long-term epilepsy associated tumors (LEAT) such as
- Dysembryoplastic neuroepithelial tumor (DNET): Wedge- or triangular-shaped, bubbly appearance, no post contrast enhancement.
- Ganglioglioma: Mixed solid and cystic appearance with, can have calcification, increased rCBV. At times, difficult to differentiate from PLNTY
- Other DDs
- Calcifying pseudoneoplasm of the neuroaxis (CAPNON) : Uniform calcified T1/T2 hypointense lesion, temporal lobe predilection. No solid enhancement
- Diffuse glioneuronal tumor with oligodendroglioma like features and Nuclear clusters (DGONC) : Seen in children (~ 9 years), focal calcifications, T2 hyperintense (ground glass signal intensity) with minimal enhancement
Treatment
Surgical resection of the tumor is curative and is associated with a low recurrence rate.
References
- Barretto BB, Mani J, Venkatraman S, Kumar A, Rao S, Kale H. Polymorphous Low-Grade Neuroepithelial Tumor of the Young (PLNTY): A Newly Described Entity of Special Radiological Significance. Indian Journal of Radiology and Imaging. 2023 Oct;33(04):567-70
- Benson JC, Summerfield D, Carr C, Cogswell P, Messina S, Gompel JV, Welker K. Polymorphous low-grade neuroepithelial tumor of the young as a partially calcified intra-axial mass in an adult. American Journal of Neuroradiology. 2020 Apr 1;41(4):573-8.
Add a Comment
You must be logged in to post a comment